

I encourage a mindset of what I call designer cataract surgery, which entails aspiring to achieve each cataract patient’s best visual potential. The femtosecond laser helps me to reach that goal even in complex cases.1-3
AT A GLANCE
• Errant capsulorrhexes prolong surgery and can lead to complications. In complex cases, the capsulotomy is therefore the most useful function of the femtosecond laser in Dr. Gulani’s opinion.
• In certain complex cases, the increased accuracy and precision of a laser capsulotomy compared with a manual capsulorrhexis can make the difference between an excellent and a poor visual outcome.
Although some surgeons continue to debate the benefits of femtosecond lasers for uncomplicated cataract procedures, I believe the technology is almost a necessity in certain complex scenarios. To me, the most important use of the laser is for the creation of the capsulotomy.4 It is this step of the cataract procedure that can pose the greatest challenge and risk in certain complex cases.5-8 Errant capsulorrhexes can prolong surgery, require a change in plans, and lead to complications such as persistent uveitis, cystoid macular edema, and secondary retinal detachment.9,10
Moreover, an irregularly shaped capsulotomy may influence the position of the IOL, leading to decentration and tilt that can decrease the patient’s quality of vision. The consistency of the laser capsulotomy can, therefore, be highly advantageous.
This article shares just three cases of many in which I found the femtosecond laser to be nearly indispensable.
Case No. 1: Torn Posterior Capsule After Retinal Surgery And White Cataract
A patient was referred to me with a dense white cataract and hand motions vision. A retina specialist had previously accidentally torn the posterior capsule while injecting an antivascular endothelial growth factor medication. The consistency of the laser for creating a capsulotomy allowed me to plan for a sulcus-based IOL, and the patient achieved a UCVA of 20/25 (Figure 1).

Figure 1. After staining the capsule with trypan blue dye, Dr. Gulani checks the capsulotomy.
Case No. 2: Cataract and Central Herpetic Corneal Scar With a Divot
I performed in-cornea laser corneoplastique on the eye of a patient with a dense, central, herpetic corneal scar and a preoperative BCVA of 20/150 (Figure 2). He was so happy with his postoperative visual acuity of 20/30 that he delayed his cataract procedure. When he presented for cataract surgery, I executed a two-step strategy, with aphakic cataract surgery followed 1 week later by the refraction-based implantation of a toric IOL (acknowledgement of Richard Mackool, MD). The patient’s UCVA improved to 20/25. The perfect, well-sized, central capsulotomy was crucial to the outcome.
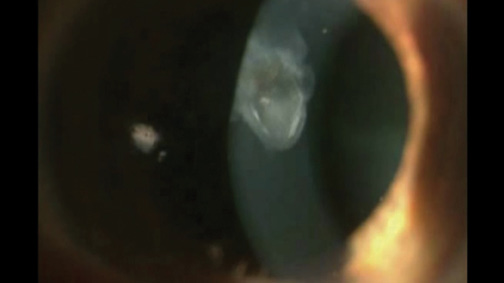
Figure 2. This patient’s eye had a dense, herpetic corneal scar, which Dr. Gulani treated with in-cornea laser corneoplastique. Later, the patient underwent a two-step cataract procedure.
Case No. 3: Nystagmus and Mature Cataract
A well-planned and well-executed capsulorrhexis in an eye with a mature cataract not only sets the stage for surgery but also decompresses the capsular bag, thus avoiding the Argentinian flag sign.
I recently treated an optician with nystagmus and a mature cataract. As I waited to dock the laser, the speculum and the patient’s eye were moving constantly. As soon as I could center the eye, I applied suction, thus controlling the nystagmus (Figure 3). Having accomplished the capsulotomy, I was then able to proceed with cataract surgery, which achieved a UCVA of 20/25.
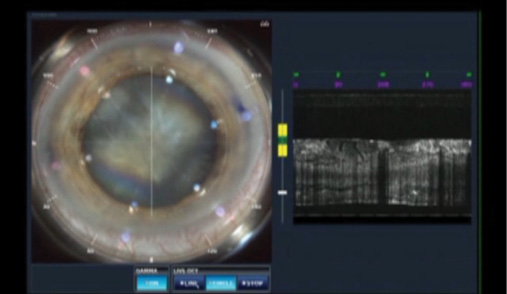
Figure 3. Dr. Gulani stabilizes the constantly moving eye of a patient who has nystagmus by applying suction the moment he can center the eye enough.
Case No. 4: Nystagmus, High Hyperopia, Fuchs Dystrophy, Small Pupils, Mature Cataract, Narrow Angle, and Shallow Anterior Chamber
An even more complex case I recently treated is a patient with nystagmus, high hyperopia (9.00 D sphere), Fuchs dystrophy, small pupils, mature cataract, narrow angle, and a shallow anterior chamber. He was also hearing impaired and had head tremors and a tracheostomy. Because the patient could not hear or speak, I knew it would be hard for him to follow my verbal orders during surgery. His head tremors caused his eyes to constantly move, which, with his very shallow anterior chamber and hypermature white cataract, would make my capsulorrhexis perilous.
Using the femtosecond laser, I was able to stabilize the patient’s moving eyes by docking him to the interface, allowing me to create a predictable capsulotomy. Thereafter, surgery was routine, leading to a predictable outcome that changed his life forever.
CONCLUSION
In complex cases such as these I have described, laser technology provides the advantage of a predictable, consistent capsulotomy. Surgical outcomes can never be guaranteed, but the increased accuracy, predictability, and precision afforded by the laser can make the difference between an excellent and a poor visual outcome for these patients.
1. Gulani AC. Femtosecond laser in refractive lens exchange: surgical treatment for presbyopia. In: Wang M, ed. Refractive Lens Exchange: A Surgical Treatment for Presbyopia Thorofare, NJ: Slack; 2016:109-115.
2. Gulani AC. Designer cataract surgery concept tailored to each case. Ophthalmology Times. July 1, 2015. http://bit.ly/1Lp3stf. Accessed October 16, 2015.
3. Gulani AC. Vision à la carte: designing vision. Ophthalmology Times. 2013;38:31-33.
4. Straub L. Evaluating the impact of femto laser-assisted capsulotomy. Cataract & Refractive Surgery Today Europe. February 2014;2(9):36-50. http://bit.ly/1Oo5HTo. Accessed October 8, 2015.
5. Bansal J, Gulani AC. Excimer laser enhancements after multifocal IOLs. In: Hovanesian J, ed. Textbook of Premium Cataract Surgery: a Step by Step Guide. 1st ed. Thorofare, NJ: Slack; 2012:135-145.
6. Donnenfeld E, Gulani AC. Astigmatism correction during cataract surgery. In: Garg H, Alió JL, eds. Femtosecond Laser: Techniques and Technology. 1st ed. Miami, FL: JayPee Highlights Medical Publishers; 2012:162-164.
7. Gulani AC. Femtosecond laser in cataract surgery: designer cataract surgery. In: Garg H, Alió JL, eds. Femtosecond Laser: Techniques and Technology. 1st ed. Miami, FL: JayPee Highlights Medical Publishers; 2012:152-154.
8. Gulani AC, Wang M. Femtosecond laser in ophthalmology: past, present and future. In: Garg H, Alió JL, eds. Textbook of Femtosecond Laser: Technology & Techniques. 1st ed. Miami, FL: JayPee Highlights Medical Publishers; 2012;22:162-164.
9. Ng DT, Rowe NA, Francis IC, et al. Intraoperative complications of 1000 phacoemulsification procedures: a prospective study. J Cataract Refract Surg. 1998;24(10):1390-1395.
10. Marques FF, Marques DM, Osher RH, Osher JM. Fate of anterior capsule tears during cataract surgery. J Cataract Refract Surg. 2006;32:1638-1642.
Arun C. Gulani, MD, MS
• Founding Director, Chief Surgeon, Gulani Vision Institute, Jacksonville, Florida
• gulanivision@gulani.com
• Financial disclosure: None provided
