

The femtosecond laser has been heralded as a revolution in cataract surgery by many and critiqued as an expensive tool for capsulorrhexis creation by some. I believe that it is in difficult and challenging situations that the advantages of this technology come to the fore.
AT A GLANCE
• In the author’s experience of more than 100 eyes with mature white and brunescent hypermature cataracts, the incidence of a free-floating capsulotomy has been greater with a liquid optics interface than with an applanating interface.
• One reason for an increased likelihood of a free- floating rhexis with the liquid optics interface is the faster rate of capsulotomy creation, as it is completed before the liquefied cortex of the intumescent cataract starts migrating into the anterior chamber.
In developing countries such as mine, it is not uncommon to encounter mature white and brunescent hypermature cataracts. The most technically demanding step of cataract surgery in white intumescent and hypermature cataracts is performing a safe continuous curvilinear capsulorrhexis. This is because difficulty in visualization due to lack of a red reflex and increased intralenticular pressure in the intumescent cataract can lead to an uncontrollable extension of the anterior lens capsule, referred to as the Argentinian flag sign.1
CAPSULOTOMY CREATION
The femtosecond laser offers the ability to create a well-centered and accurately sized capsulotomy with precise effective lens position and superior postoperative visual outcomes, even in challenging cases.2 In our experience of more than 100 eyes with mature white and brunescent hypermature cataracts, the incidence of a free-floating capsulotomy is greater with a liquid optics interface as opposed to an applanating interface, due to reduced distortion of the cornea and relatively uninterrupted passage of the femtosecond laser with use of the former (Figure 1). Therefore, I prefer laser-assisted cataract surgery (LACS) in such cases.
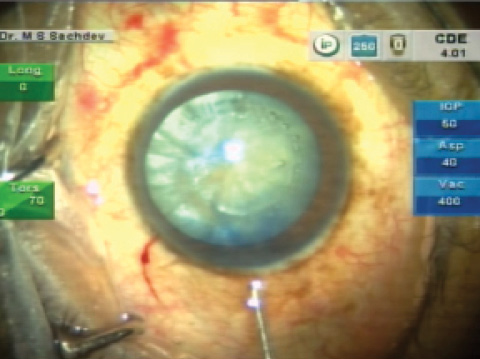
Figure 1. Free-floating capsulotomy in a mature cataract.
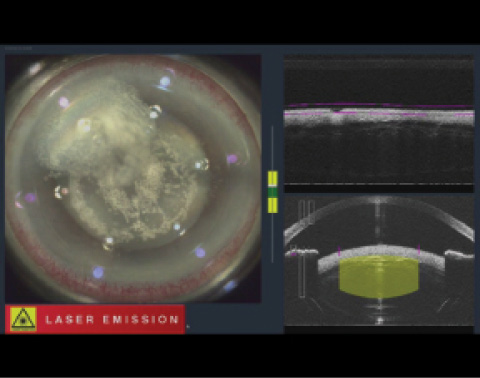
Figure 2. Egress of cortical fluid after commencement of capsulotomy.
The faster rate of capsulotomy formation with the liquid optics interface may also contribute to the increased probability of achieving a free-floating rhexis, as it is completed before the liquefied cortex of the intumescent cataract starts migrating into the anterior chamber. Additionally, the anterior and posterior offsets for the capsulorrhexis can be increased from the usual limit of 250 µm—up to 1,000 µm—which can help to achieve a complete cut despite any distortions of the capsular surface that may happen due to egress of milky cortical matter.
Although free-floating capsulotomies can often be achieved, it is wise to anticipate the presence of microadhesions of the capsulotomy in such cases. Increased intracapsular pressure results in partial collapse of the anterior lens surface in the area of breakthrough during the laser application, and, consequently, areas of the capsulotomy can remain uncut.
Moreover, egress of the liquefied lens material into the anterior chamber can result in a compromised capsulotomy and increased difficulty of subsequent lens fragmentation (Figure 2). Lateral movement of the anterior capsule due to raised tension on the opposite side may lead to an incomplete cut of the capsulotomy or application of the laser more centrally than expected. Uncut areas may also be noted in regions of capsular calcification and fibrosis, which are common in hypermature cataracts.
Trypan blue dye can be used to stain the capsule and to facilitate assessment for the presence of capsular tags or small adhesions.
The detached capsulorrhexis should be pulled to the center in a curvilinear fashion before removal. A dimple-down technique has also been described to ensure that the capsule is separated completely before it is removed with forceps. These simple steps allow the surgeon to achieve a continuous capsulotomy without extension from any of the uncut areas.
ADDRESSING THE NUCLEUS
Nucleus disassembly represents the next challenge in brunescent cataracts. Lens fragmentation and softening in hard cataracts result in reduced effective phacoemulsification time and lower energy use, leading to reduced incidence of postoperative corneal edema. A more compact than usual grid spacing of 200 µm is preferred in these cases; selection of six- to eight-segment femtosecond laser cuts further enhances the ease of nuclear breakdown.
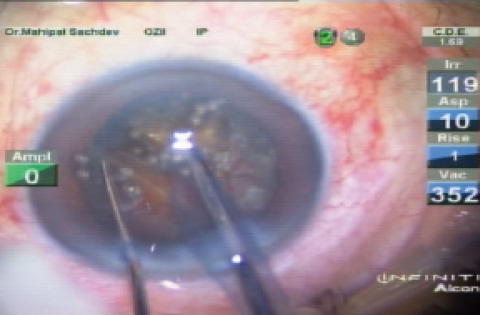
Figure 3. Lens fragmentation in a grade 5 cataract.
Due to limited penetration of femtosecond laser pulses through opaque tissue, the efficacy of lens fragmentation in white cataracts is limited. Nevertheless, in most cases, the laser provides sufficient grooving to aid in subsequent chopping and emulsification of the nucleus (Figure 3).
Imaging of the posterior lens capsule is also difficult in these cases, as the OCT-guided imaging does not penetrate through the white cataract. Therefore, adjustment of the posterior capsular offset must be made manually.
Create a Foundation for Precision
No. 1: Anticipate the presence of microadhesions of the capsulotomy.
No. 2: Egress of the liquefied lens material into the anterior chamber can result in tags or microadhesions in the capsulotomy and limited lens fragmentation.
No. 3: Trypan blue dye staining to enhance visualization, pulling of the detached capsulorrhexis to the center in a curvilinear fashion, and a dimple- down technique can help to achieve a continuous capsulotomy without extension from any of the uncut areas, which can occur in regions of capsular calcification and fibrosis.
No. 4: Six- to eight-segment femtosecond laser cuts can enhance the ease of nuclear breakdown.
No. 5: Burp out any air bubbles that may be trapped behind the nucleus, as pneumodissection in harder cataracts is more extensive.
Before performing hydrodissection, it is important to burp out any air bubbles that may be trapped behind the nucleus, as pneumodissection in harder cataracts is more extensive. This ensures that further increase in intralenticular pressure, which could lead to disastrous complications such as posterior capsular blowout, is prevented.3
The grooves created by the femtosecond laser enable a direct chop to be performed with relative ease, even in hard cataracts. The additional softening caused by the laser greatly reduces the effective phacoemulsification time and helps to achieve a clear cornea on postoperative day 1.
CONCLUSION
I have found that LACS is a useful adjunct in complicated cases including intumescent and white cataracts. With that said, one must be mindful of five key points that encourage a solid foundation for enhanced surgical control and successful postoperative results in eyes with mature and hard cataracts (see Create a Foundation for Precision). Looking at the big picture, LACS can help improve the efficacy and safety of cataract surgery and also reduce the rate of complications.
1. Conrad-Hengerer, Hengerer FH, Joachim SC, et al. Femtosecond laser-assisted cataract surgery in intumescent white cataracts. J Cataract Refract Surg. 2014;40:44-50.
2. Friedman NJ, Palanker DV, Schuele G, et al. Femtosecond laser capsulotomy. J Cataract Refract Surg. 2011;37(7):1189-1198. Erratum in: J Cataract Refract Surg. 2011;37(9):17.
3. Roberts TV, Lawless M, Bali SJ, Hodge C, Sutton G. Surgical outcomes and safety of femtosecond laser cataract surgery; a prospective study of 1500 consecutive cases. Ophthalmology. 2013;120:227-233.
Mahipal S. Sachdev, MD
• Chairman and Medical Director, Centre For Sight Group of Eye Hospitals, New Delhi, India
• drmahipal@gmail.com
• Financial disclosure: Travel support (Abbott Medical Optics)
