

Today, with the use of small incisions and foldable IOLs, cataract extraction has become a safer and more effective surgery than ever. However, despite many advances over the years, the current state of cataract surgery nevertheless involves safety concerns and refractive limitations. Complications such as endophthalmitis, posterior capsular rupture, and cystoid macular edema still arise. Refractive accuracy remains suboptimal, and true accommodating IOLs are in their first generation with much advancement yet to come.
AT A GLANCE
• The use of the femtosecond laser can simplify cataract surgery and reduce complications in challenging cases and can also offer the surgeon a way to perform surgical maneuvers that are impossible to perform manually.
• The imaging capabilities of the femtosecond laser allow surgeons to visualize lens tilt, vitreous presentation, anterior chamber depth, and lens thickness—information that can be invaluable in complex cataract surgery cases.
• With LACS, traumatic capsulotomies and lens disruption can now be performed even in eyes after trauma, despite zonular dehiscence and vitreous in the anterior chamber.
Most important, we continue to be challenged by complex eyes, such as those with weak zonules, partially dislocated crystalline lenses, low endothelial cell counts, shallow anterior chambers, and mature lenses. The use of the femtosecond laser can significantly simplify and reduce complications in these challenging cases. Additionally, the femtosecond laser can perform surgical maneuvers that are simply impossible to perform manually. The true test of the femtosecond laser for cataract surgery is its ability to improve outcomes in the most difficult cases that all cataract surgeons deal with on a routine basis.
A major advantage of femtosecond laser technology is the imaging capability incorporated into these systems. Femtosecond laser systems include built-in OCT or Scheimpflug imaging that allows us to measure the relevant dimensions of the anterior segment, namely the cornea, the anterior and posterior lens capsules, and the nucleus (Figure 1). Based on these measurements, the laser-assisted cataract surgery (LACS) treatment can be planned and performed. This imaging ability allows surgeons to visualize lens tilt, vitreous presentation, anterior chamber depth, and lens thickness—information that can be invaluable in complex cataract surgery cases. Preoperative knowledge of the crystalline lens dimensions provides the surgeon with useful information in cataract surgery planning.
This article examines some specific complex issues in cataract surgery in which femtosecond technology represents an improvement over manual surgery.

Figure 1. OCT imaging of the anterior segment demonstrates the position and size of the cataract.
CAPSULOTOMY CREATION
Capsulorrhexis creation is one of the most important and occasionally challenging steps in cataract surgery. A round, adequately sized, and well-centered capsular opening ensures proper centration of the IOL, and its durability allows complicated movements to be performed during phacoemulsification. However, capsulorrhexis creation is variable, depending on the experience of the surgeon and patient-specific factors such as pupil dilation and anterior chamber depth. A single radial tear from the capsulorrhexis introduces significant risk of extension to the posterior capsule.
The ability of the femtosecond laser to make a rapid capsulotomy before the eye is opened means the physiologic pressure differential between the anterior and posterior chambers is maintained, reducing the tendency of the lens to push forward due to positive vitreous pressure or intumescence. The Argentinian flag sign can occur when a capsulotomy is made in an anterior capsule stained with gentian blue dye; low pressure in the anterior chamber causes the lens to move forward, creating a radial tear in the anterior capsule.
CAPSULOTOMY IN HIGH-RISK CASES
MATURE LENSES
Although the laser will not penetrate through a white intumescent lens (Figure 1), its ability to create a capsulotomy in these lenses with reduced risk of a radial tear is a significant advantage.
TIGHT SPACES
The laser allows capsulotomy creation in patients with shallow anterior chambers, which may be difficult to perform manually (Figure 2).
LOOSE LENSES
In patients with poor zonular support, capsulotomy may not only be challenging but may also cause additional zonular damage. In eyes with an acquired or congenital lens dislocation, the femtosecond laser can penetrate through vitreous in the anterior chamber to perform a successful capsulotomy.
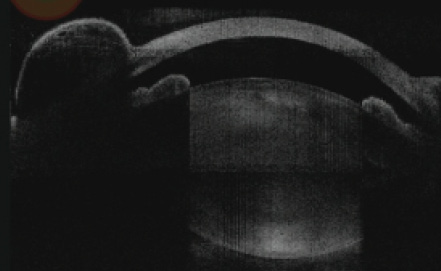
Figure 1. Femtosecond laser technology allows safer capsulotomy creation in a white intumescent cataract.
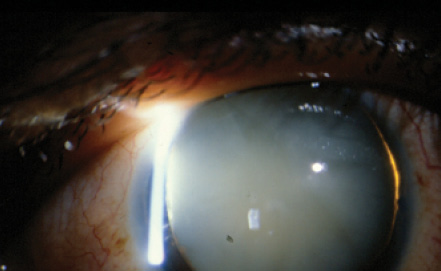
Figure 2. Shallow anterior chamber in a patient with a dense cataract after trabeculectomy. Femtosecond capsulotomy is safer than manual capsulorrhexis in such patients.
With the femtosecond laser, capsulotomy creation is significantly safer in many types of high-risk cases (see Capsulotomy in High-Risk Cases). In each of these complicated and challenging situations, femtosecond laser can perform a capsulotomy seamlessly.
REDUCED ENERGY
Another limiting aspect of conventional cataract surgery in difficult cases is the duration and intensity of phacoemulsification time required and its impact on corneal endothelial cell count. Significantly greater phacoemulsification energy is needed to emulsify the crystalline lens when laser fragmentation is not performed, and the additional energy is associated with a loss of endothelial cells.
The femtosecond laser reduces or eliminates the need for phacoemulsification in many lenses. Femtosecond lasers are photodisruptive lasers with extraordinarily short pulse durations of less than 800 femtoseconds (1 femtosecond is 10-15 seconds). This extremely short pulse duration allows femtosecond lasers to cut tissue with considerably less energy than traditional lasers used in other aspects of ophthalmic surgery.
Nagy et al performed ex vivo studies of femtosecond laser in porcine eyes.1 After femtosecond phacofragmentation, average phaco power was reduced by 43% (P<.001) and effective phaco time (EPT) by 51% (P<.001) compared with standard phacoemulsification. Batlle et al demonstrated a 40% reduction in cumulative dispersive energy in eyes pretreated with the laser, compared with the traditional approach.2
Edwards et al have also shown an absolute decrease in energy required proportional to the grading of the cataract, with a statistically significant decrease for grades 1 and 2 cataract.3 In a clinical setting, Mayer et al showed that LACS significantly reduced EPT compared with manual phacoemulsification.4 Less EPT resulted in clearer corneas, less endothelial cell loss, and better safety. A paper by Conrad-Hengerer and colleagues reported that the use of the femtosecond laser can eliminate phacoemulsification energy in most mild to moderate cataract surgeries.5
The femtosecond laser is also helpful in reducing EPT and endothelial cell loss in challenging dense cataracts. In a study by Hatch et al, femtosecond laser pretreatment of brunescent cataracts allowed significant reduction in EPT compared with conventional phacoemulsification techniques.6
CONCLUSION
Although still in its infancy, LACS has already been shown to produce more reliable and accurate capsulotomies while reducing phaco energy and phaco time. Reducing intraocular application of energy reduces the risk of endothelial cell loss, which should make the cataract surgical procedure safer for all patients—but particularly for patients with compromised endothelium such as in Fuchs dystrophy. Additionally, with femtosecond laser, less stress is placed on the patient’s zonules, which is ideal for patients with compromised zonular support, such as those with pseudoexfoliation or a history of accidental or surgical trauma.
We have witnessed the natural progression of cataract surgery from intracapsular, to extracapsular, to phacoemulsification, and now to the femtosecond laser. The future of cataract surgery will lie in our ability to correct the limitations we currently have and produce a more optimized cataract extraction procedure. Atraumatic capsulotomies and lens disruption can now be performed even in eyes after trauma, despite zonular dehiscence and vitreous in the anterior chamber.
Less energy applied inside the eye will increase the safety of the procedure, reduce endothelial cell loss, and reduce the risk of lens dislocation in patients with compromised zonules. This technology currently improves safety in complex cases and will improve it further in the near future. LACS is a novel technique that provides the precision of image-guided laser technology. It will dramatically elevate the level of cataract surgery for all surgeons and improve safety and efficacy in the most challenging cases we perform.
1. Nagy Z, Takacs A, Filkorn T, et al. Initial clinical evaluation of an intraocular femtosecond laser in cataract surgery.
J Refract Surg. 2009;25:1053-1060.
2. Batlle JF, Feliz R, Culbertson WW. OCT-guided femtosecond laser cataract surgery: precision and efficacy. Poster presented at: Association for Research in Vision and Ophthalmology Annual Meeting; May 1-5, 2011; Fort Lauderdale, Florida.
3. Edwards K, Uy HS, Schneider S. The effect of laser lens fragmentation on use of ultrasound energy in cataract surgery. Poster presented at: the Association for Research in Vision and Ophthalmology Annual Meeting; May 1-5, 2011; Fort Lauderdale, Florida.
4. Mayer WJ, Klaproth OK, Hengerer FH, Kohnen T. Impact of crystalline lens opacification on effective phacoemulsification time in femtosecond laser-assisted cataract surgery. Am J Ophthalmol. 2014;157:426-432.e1.
5. Conrad-Hengerer I, Hengerer FH, Schultz T, Dick HB. Effect of femtosecond laser fragmentation on effective phacoemulsification time in cataract surgery. J Refract Surg. 2012;28(12):879-883.
6. Hatch KM, Schultz T, Talamo JH, Dick HB. Femtosecond laser-assisted compared with standard cataract surgery for removal of advanced cataracts. J Cataract Refract Surg. 2015;41(9):1833-1838.
Eric D. Donnenfeld, MD
• Professor of Ophthalmology, New York University
• Trustee, Dartmouth Medical School, Hanover, New Hampshire
• Member, CRST Europe Global Advisory Board
• ericdonnenfeld@gmail.com
• Financial disclosure: Consultant (Abbott Medical Optics, Alcon, Bausch + Lomb)