

Dislocated lenses present great challenges for surgeons, including the questions of when is the best time for surgery and what is the best approach intraoperatively. Because we have now have had positive experiences with use of femtosecond laser in these cases, we tend to do the operation earlier than we did before.
AT A GLANCE
• In a dislocated lens, manual capsulorrhexis causes additional stress to the zonula; femtosecond laser capsulotomy can be performed without placing any additional stress on the zonula, and the capsulotomy can be removed without additional forces.
• LACS in a dislocated lens offers the possibility of standardized treatment and can allow earlier treatment with fewer complications and better results.
We believe surgery for the dislocated lens is indicated in a number of situations, which are listed in the graphic below.
common cause: MARFAN SYNDROME
In our clinic, for many of the patients we see with dislocated lenses, the cause is Marfan syndrome. This is a systemic disorder of the connective tissue brought about by a genetic mutation. It can occur as an autosomal dominant (70%) or a new mutation (30%). Symptoms include problems with the eye, in particular dislocation of the crystalline lens or cataract.
The most difficult part of cataract surgery in dislocated lenses is without doubt the capsulotomy. Manual capsulorrhexis causes additional stress to the zonula, which may lead to more damage intraoperatively and, if the damage is too severe, complete loss of the lens or the capsular bag. Often vitrectomy is necessary, making surgery even more traumatic.
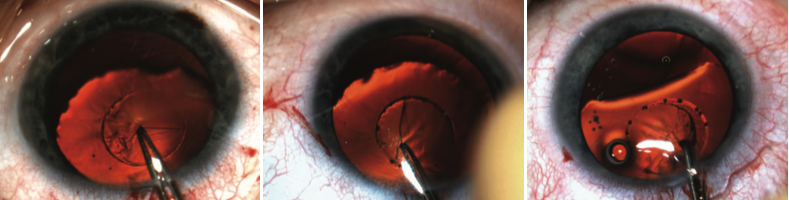
Figure 1. The tag of a laser-assisted capsulotomy is removed in an eye with a dislocated lens.
Femtosecond laser capsulotomy, on the other hand, can be performed without placing any additional stress on the zonula, and the capsulotomy can be removed without additional forces (Figure 1). The opening will have the planned size and location—another advantage compared with manual capsulorrhexis.
LASER DEBUT
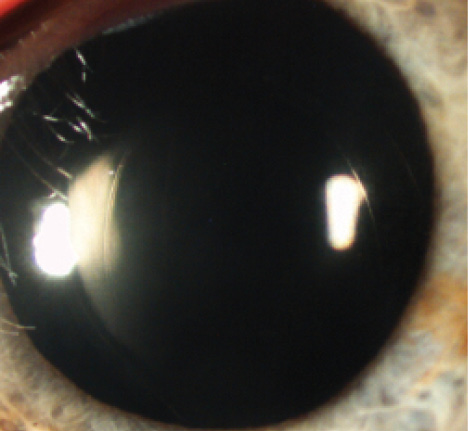
Figure 2. Postoperative outcome in an eye with a dislocated lens that underwent LACS.
In 2013 we performed the world’s first laser-assisted cataract surgery (LACS) with the Lensar Laser System (Lensar). The surgery was in a dislocated lens in a 23-year-old man with Marfan syndrome.
The capsulotomy was centered on the lens apex. Due to the young age of the patient, no fragmentation was performed, and the lens was aspirated without ultrasound energy. An 11-mm diameter capsular tension ring (Morcher type 1L) was inserted and sutured to the sclera at the 6-o’clock position. A hydrophilic one-piece IOL was implanted through a 2.4-mm limbal incision into the capsular bag.
With 3 years’ experience, we have now performed LACS in eight eyes with dislocated lenses using the same technique (Figure 2). In all cases the capsulotomy was performed without complication and no adverse events occurred intra- or postoperatively. The capsule was removed without additional stress to the zonula. Visual acuity recovered quickly, and refractive error (ie, lens-induced myopia and astigmatism) decreased.
Indications for LACS in Eyes With Dislocated Lenses
• If the patient’s refraction changes quickly
• If greater lens-induced myopia and astigmatism are seen
• If visual acuity decreases
• If the dislocation of the lens becomes more severe from one visit to the next; to detect this, a comparison of slit-lamp photographs is helpful
In some severe cases, the capsulotomy could not be performed by the laser because the opening could not be located at a safe distance from the edge of the lens. For cases such as these, it would be helpful if the surgeon could move the capsulotomy to the desired position using a drag-and-drop method on the Lensar’s touchscreen.
Fragmentation of the lens was also performed in some cases. This was planned in a small central zone and, because of the young age of the patients, with chops in only two planes.
After our good experiences in these cases, Lensar created an extended scan mode in the device’s software, which allows additional scans for more safety in the 3-D reconstruction of the eye.
CONCLUSION
Laser-assisted capsulotomy of a dislocated lens is a gentle and safe method. It offers the possibility of standardized treatment and will lead to earlier treatment with fewer complications and better results in these challenging cases.
Detlef Holland, MD
• nordBLICK Augenklinik Bellevue, Kiel, Germany
• CRST Europe Editorial Board member
• mailto:d.holland@nordblick.de
• Financial disclosure: Consultant (Lensar)
