
Optimal Capsular Staining Calls for High-Purity Vital Dye
Injections of an air bubble and OVD help to achieve best results.

By Elena Barraquer, MD
My principal practice is in Barcelona, Spain, but I also perform about 1,500 cataract surgeries a year in Africa. Most of these cases require anterior capsule staining because they involve mature cataracts. Simply put, I could not operate efficiently in mature cataracts without trypan blue vital dye.
Even in more routine cases, staining the anterior capsule with VisionBlue capsular dye (trypan blue ophthalmic solution 0.06%; DORC International) during cataract surgery is often necessary for better visualization. This is true not only in advanced cataracts, but also in other conditions in which there is insufficient red fundus reflex and the coaxial microscope light does not adequately identify the anterior capsule. For example, if a cataract patient is scheduled to undergo vitreoretinal surgery for diabetic vitreous hemorrhage, even with a normal cataract the surgeon may not be able to identify the anterior capsule optimally because of the lack of red reflex.
CONSIDERATIONS IN SELECTING A STAIN
My preferred staining approach in cataract surgery is to use VisionBlue. Some ophthalmic trypan blue solutions include clumps, and, in my experience, these may not stain the anterior capsule optimally. In instances in which this has happened, it can compromise the entire procedure. This is especially true if the capsule is fibrotic in some spots, as the surgeon may not be able to visualize a capsulorrhexis continuation in an unwanted direction, and posterior capsular disruption can result.
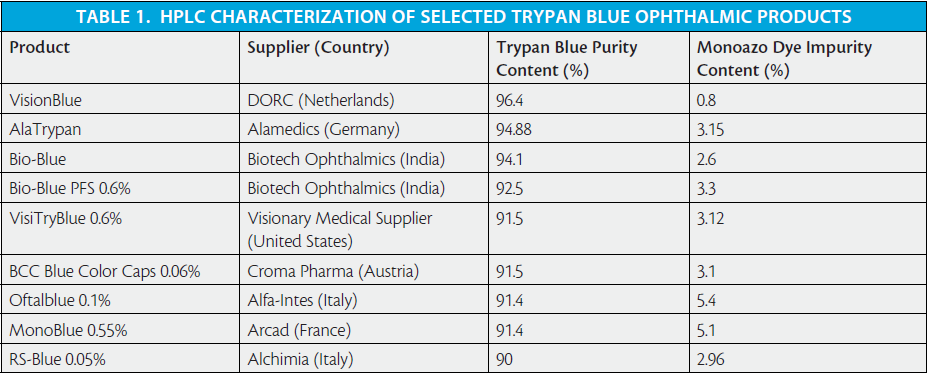
I look for maximum purity in an ophthalmic staining liquid so that I can be confident that the injected vital dye will not damage the corneal endothelium. The purity of any substance injected into the anterior chamber must be extremely high; if not, it may be toxic to the corneal endothelium (see Comparative HPLC Characterization of Selected Trypan Blue Ophthalmic Products).
Toxic anterior segment syndrome (TASS) can occur as a result of intraocular use of products containing impurities.1 An outbreak of TASS can affect all patients undergoing surgery in a single clinic session. In Africa, where we operate on 40 cataract patients in 1 day, it would be disastrous to have an outbreak of TASS.
In addition to purity and safety considerations, it is equally important that the anterior capsule be stained in a homogeneous manner, which is not the case with all trypan blue formulations. If the entire anterior capsule is not stained sufficiently, the surgeon may encounter difficulties such as losing one’s grip on the anterior capsulotomy edge, thereby risking a discontinued capsulorrhexis. This can progress to a defect in the posterior capsule and make it difficult to implant an IOL securely.
OPTIMAL STAINING TECHNIQUE
Injection of an air bubble prior to dye instillation is an important step to help obtain good capsular staining. Using the same syringe, I first inject an air bubble and, immediately after that, between the bubble of air and the anterior capsule, I inject VisionBlue. Just a few drops of dye are sufficient to effectively stain the anterior capsule throughout. Then I inject an OVD, which helps to fix the dye to the anterior capsule.
At a Glance
• Staining quality and safety are the principal issues in selecting an appropriate dye to stain the capsule during anterior segment surgery.
• The main benefits of trypan blue staining in cataract surgery are enhanced visualization of the anterior lens capsule and a low incidence of complications.
• The use of trypan blue ophthalmic solution as a selective tissue staining agent extends to other anterior segment surgeries beyond cataract extraction, including lamellar corneal surgery.
1. Mamalis N, Edelhauser HF, Dawson DG, Chew J, LeBoyer RM, Werner L. Toxic anterior segment syndrome. J Cataract Refract Surg. 2006;32(2):324-333. Review.
High-Performance Liquid Chromatography Characterization of Trypan Blue Ophthalmic Products
1. Data on file, DORC International.
Capsular Staining is Helpful in Routine and Complex Cases
Safety is paramount.
By Thamotharan S. Naidu, MD
Capsular staining with trypan blue ophthalmic solution can be helpful in multiple situations: in dense cataracts for better visualization; in the presence of a small pupil; and for beginning surgeons, to simplify the processes of learning and training. Safety is paramount, and using VisionBlue capsular dye for initial visualization of the anterior capsule at the start of cataract surgery makes the procedure significantly easier and safer than without the use of dye.
In my surgical practice, lens capsule staining is carried out in approximately 80% to 90% of cataract cases. The use of a selective tissue-staining agent has become an everyday practice for performing anterior capsulotomy, whether for routine cases or complex cases that involve combined intraoperative procedures.
Anterior capsule staining simplifies the performance of the surgical procedure and helps to minimize adverse events. Intraoperative complications such as loss of the capsulorrhexis are rare. I cannot recall a case in which I have lost the capsulorrhexis radially while using trypan blue dye; this is because visualization of the capsule is perfect. This enhancement leads to massive reduction in the frequency of radial tears during capsulorrhexis.
In my experience using VisionBlue for anterior segment surgery, there is limited risk of postoperative cystoid macular edema (CME) or severe intraocular inflammation.
RAPID STAINING EFFECT, ENHANCED INTRAOPERATIVE VISUALIZATION
After injection under an air bubble and application directly on the anterior lens capsule, the ophthalmic solution stains as soon as the dye contacts the capsule. Excess dye is immediately washed from the eye by thorough irrigation of the anterior chamber. Once the rhexis is folded over, visualization remains excellent.
Some colleagues use trypan blue ophthalmic solution for staining the capsule in highly dense cataract cases only, and others use it as a staining agent for almost all cataract procedures. I fall into the latter category.
The main benefits of trypan blue staining are enhanced visualization of the anterior lens capsule and a low incidence of complications. Absolute clarity of visualization of the anterior chamber is the first essential requirement for the creation of a continuous curvilinear capsulorrhexis. There is no risk of loss of the capsule, which can typically be a risk when operating under a smaller pupil.
Using trypan blue dye for staining the anterior capsule of the human crystalline lens during cataract surgery represents a major contribution to the achievement of better clinical outcomes, at least in my hands. Anterior staining improves overall safety and represents a valuable surgical aid in securing sound, predictable completion of the capsulorrhexis procedure in cataract surgery.
Considerations and Approaches in Dye-Assisted Anterior Segment Surgery Beyond Cataract Extraction
Membrane staining can improve lamellar corneal transplant procedures.

By Francis W. Price Jr, MD
Anterior segment staining using trypan blue vital dye has made many potentially complicated cases of cataract surgery significantly safer. Trypan blue dye is used routinely to stain the anterior capsule of the crystalline lens, which is important in eyes with white cataract or with no or poor red fundus reflex. Staining aids in visualization of the lens capsule, allowing the cataract procedure to be performed safely and efficiently.
Assured quality and performance are the reasons we use only VisionBlue, a licensed trypan blue ophthalmic solution with a proven track record. We know how it works, how quickly it works, and the relevant toxicity considerations, such as avoiding use of high concentrations for extended periods of time.
OTHER USES
We use VisionBlue for capsule and membrane staining in other anterior segment surgical procedures in addition to cataract surgery. Several of these applications are detailed below.
Iris reconstruction. We use trypan blue dye in complicated anterior segment reconstructions involving artificial iris implantation. Iris reconstruction implants for complete and partial aniridia include ArtificialIris (HumanOptics), an acrylic, foldable 9-mm diameter optic small-incision iris prosthesis, and Aniridia 311 lens (Ophtec), a PMMA lens for correction of aniridia and iris coloboma.
When iris reconstruction is performed in combination with cataract surgery, the artificial iris implant can be placed in the capsular bag, provided that the capsule is stable. It is more or less essential to stain the capsular membrane before attempting to put an artificial iris implant in the bag. VisionBlue is injected after cataract removal to stain the capsular membrane; this helps to ensure that the artificial iris implant is placed completely behind the anterior capsule, directly into the capsular bag.
Endothelial keratoplasty. The use of trypan blue dye for vital staining has made a sizeable improvement in our ability to reliably carry out endothelial keratoplasty for the treatment of corneal endothelial dysfunction. VisionBlue is used to achieve intense membrane staining during stripping and scoring of Descemet membrane for Fuchs corneal endothelial dystrophy. This allows the surgeon to visualize any retained Descemet membrane to ensure removal of guttae in the pupillary area during Descemet stripping endothelial keratoplasty (DSEK)—a step that is necessary to avoid decreased vision, glare, and haze that can result from residual guttae. In our practice protocol, we use VisionBlue to identify localized areas of Descemet membrane that have not been removed and to check for loose pieces of membrane or stroma.
Especially during Descemet membrane endothelial keratoplasty (DMEK), which involves the implantation of donor endothelium and Descemet membrane, care is needed to ensure that there is no loose stroma, as this could prevent effective graft attachment. We stain the donor Descemet membrane, usually for about 1 minute, and this allows the surgeon to visualize the donor tissue clearly and to check orientation during corneal transplantation.
The donor Descemet membrane typically curls up, and, when it does, the donor endothelium is always on the outside. It is important not to traumatize the endothelium and to ensure that the donor membrane is positioned correctly on the back of the recipient cornea. It is therefore essential during DMEK to be able to properly visualize the donor tissue. If the donor membrane is stained appropriately, then there is excellent visualization of the donor endothelium and Descemet membrane through the cornea.
IMPROVED OUTCOMES
In a comparative case series evaluation, we found that the risk of corneal transplant rejection was significantly reduced after DMEK compared with DSEK and PKP.1,2 The cumulative risk for a graft rejection episode through 2 years after DMEK was one-twentieth that for similar indications for penetrating keratoplasty, and one-fifteenth that for eyes treated with DSEK.
DMEK represents a major benefit for patients in terms of better functional vision, significantly lessened risk of graft rejection after surgery, and reduced likelihood of steroid-induced glaucoma due to reduced steroid use after DMEK. (Editor’s Note: See Standardized No-Touch DMEK for Beginners, on page 78, for more information on the benefits of DMEK.) Intraoperative anterior segment OCT may also be useful to help with graft orientation, but, even here, staining the donor tissue is necessary to achieve good visibility on OCT scans.
CONCLUSION
So long as trypan blue dye is used appropriately, excellent results are achievable in anterior segment surgery, including endothelial keratoplasty. VisionBlue has made it better for our patients, and that is the whole reason we use it. It provides an effective surgical stain without unwanted prolonged staining. Its availability has also aided the evolution of endothelial keratoplasty and facilitated broader adoption of DMEK for restoration of the cornea.3 n
1. Anshu A, Price MO, Price FW Jr. Risk of corneal transplant rejection significantly reduced with Descemet’s membrane endothelial keratoplasty. Ophthalmology. 2012;119(3):536-540.
2. Price MO, Price FW Jr. Descemet’s membrane endothelial keratoplasty surgery: update on the evidence and hurdles to acceptance. Curr Opin Ophthalmol. 2013;24(4):329-335.
3. Price FW Jr, Price MO. Evolution of endothelial keratoplasty. Cornea. 2013;32 Suppl 1:S28-32.
Elena Barraquer, MD
• Associate Medical Director, Barraquer Ophthalmology Center, Barcelona, Spain
• ebarraquer@barraquer.com
• Financial disclosure: None
Thamotharan S. Naidu, MD
• Ophthalmologist and Ophthalmic Surgeon, Life Mount Edgecombe Hospital, Phoenix, Durban, South Africa
• ts_naidu@telkomsa.net
• Financial disclosure: None
Francis W. Price Jr, MD
• Ophthalmic Surgeon and President, Price Vision Group & Cornea Research Foundation of America, Indianapolis, Indiana
• fprice@pricevisiongroup.net
• Financial disclosure: None
