



Patients today are increasingly demanding when it comes to their expectations regarding cataract surgery. They want the maximum degree of intraoperative safety with fast visual recovery and excellent—if not perfect—visual acuity without glasses. In order to deliver, surgeons must use every technique, instrument, and device available.
Two of the newest (and not mutually exclusive) instruments that have been added to our arsenal are femtosecond (LenSx Laser System; Alcon) and nanosecond (Cetus Nano-Laser-System; A.R.C. Laser) lasers. The former can be used in femtosecond laser-assisted cataract surgery (LACS) to perform several steps robotically,1-3 and the latter can be used as a substitute for phacoemulsification. In order to use them correctly, we must know the advantages that each can give in terms of quality and quantity of vision, as well as their disadvantages.
AT A GLANCE
• Two of the newest (and not mutually exclusive) instru- ments that have been added to cataract surgeons’ arse- nal are femtosecond and nanosecond lasers.
• In order to use femtosecond and nanosecond lasers correctly, surgeons must know the advantages that each can give in terms of quality and quantity of vision as well as their disadvantages.
• The femtosecond laser can be used in LACS to perform several steps robotically, and the nanosecond laser can be used as a substitute for phacoemulsification.
FEMTOSECOND LASER: ADVANCES
Recently developed femtosecond laser fragmentation patterns (dice or cube). Such patterns yield crystalline lens cubes that are approximately the size of the phacoemulsification tip’s aperture, thus reducing the amount of energy needed to remove the lens.
Creation of laser-assisted clear corneal incisions (CCIs). CCIs made with a femtosecond laser consistently show a multiplanar architecture that provides a greater degree of stability than single-plane incisions. This correlates with lower variability in surgically induced astigmatism and improved postoperative visual performance. The improved geometry of CCIs also promotes self-sealing of incisions, reducing the risk of postoperative infection.3,4
IOL position. Capsulotomies performed with a femtosecond laser are more circular and symmetrical than manual capsulorrhexes, with a preset diameter permitting consistent overlap of the rhexis over the IOL edge. This allows better positioning of the IOL within the capsular bag with less decentration and tilting of the lens over time. The accuracy of positioning is particularly important with premium IOLs, such as multifocal and toric lenses. Several studies have reported less increase in higher-order aberrations in patients undergoing LACS than manual surgery.5,6
Despite these advantages, caution is advised with this technology. Recent studies have reported that increasing the total energy used for capsulotomy and CCI, even using the same femtosecond laser system, was correlated with greater tissue trauma, increasing inflammation, and tissue apoptosis.7,8
Additionally, although use of the femtosecond laser improves outcomes and reduces mechanical trauma, it also introduces a greater amount of energy (especially heat) within a closed system. Although the heat is readily dispersed, because the system remains closed for a variable time as the procedure progresses, any inflammation-inducing substances that are produced will persist.9 Overall, the total amount of energy introduced to the eye is lowered because the amount of phacoemulsification energy subsequently required for lens fragmentation is significantly reduced, and, thus, corneal edema and endothelial cell loss are also reduced.10,11
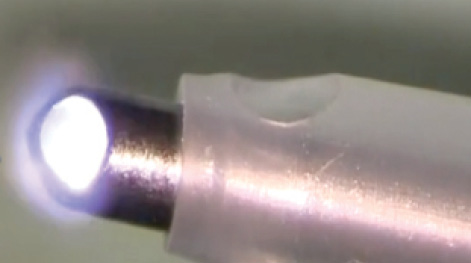
Figure 1. The rounded tip of the nanosecond laser handpiece.
NANOSECOND LASER: ADVANTAGES
The newest addition to our arsenal is a nanosecond laser, which can replace the use of phacoemulsification for cataracts of up to grade 3. The Cetus system is composed of a base that contains the laser and an optical fiber that transmits the laser impulses to a disposable one-use coaxial handpiece. The base unit can be connected to any phaco I/A system and controlled by the footpedal for that system; thus, the controls remain familiar to the surgeon. The tip of the handpiece can be fitted with the surgeon’s choice of sleeves of two diameters: 2.2 and 2.6 mm.
The laser is a 4- to 5-ns pulsed, 1064-nm wavelength Nd:YAG laser with a pulse frequency of up to 10 Hz. The individual pulse energy can be varied from 3 to 10 mJ, and the system reports the total energy used during the procedure in millijoules. Lens fragmentation is performed via a process of photofragmentation induced by the laser pulse striking a titanium plate located near the aperture in the rounded tip at a 45° angle.
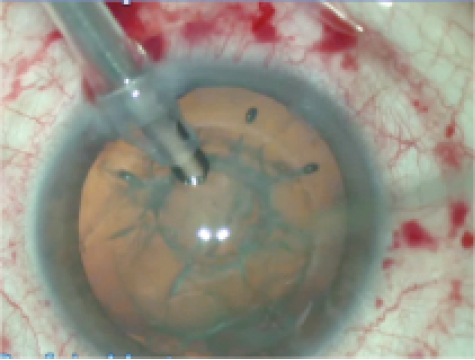
Figure 2. Emulsification of the crystalline lens with the nanosecond laser after femtosecond laser fragmentation.
The advantages of this system are numerous.
The laser pulse travels via an optical fiber. This fact guarantees minimal transfer of heat to surrounding tissue, thus reducing corneal edema even in relatively long procedures.
The laser’s design. The rounded tip and aperture borders greatly reduce the risk of posterior capsular damage (Figure 1). The single-use handpiece decreases the risk of endophthalmitis.
CLINICAL EXPERIENCE
Several authors have evaluated the effectiveness of the nanosecond laser in cataract surgery. A. John Kanellopoulos, MD, one of the first to publish a study using nanosecond laser energy for cataract surgery, reported that the system was safe and effective for the removal of cataracts up to grade 3 with an average energy value of 5.65 J per patient, which was lower than that required for phacoemulsification. The nanosecond laser procedures were also associated with a reduced rate of intraoperative complications.12
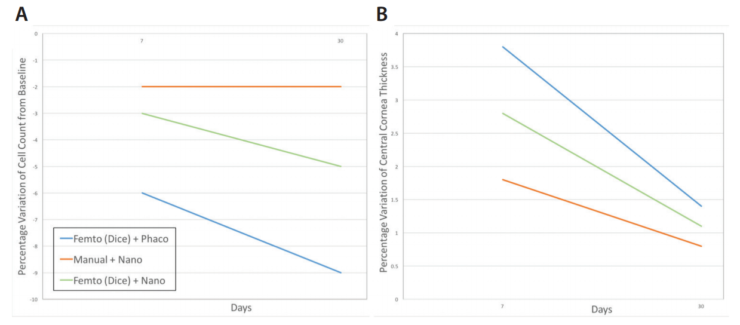
Figure 3. Endothelial cell loss (A) and central corneal thickness (B) at 7 and 30 days after femto + phaco, manual + nano, and femto + nano surgery.
With the introduction of the femtosecond laser in cataract surgery, the same author later evaluated the efficacy of surgery combining femtosecond and nanosecond lasers. He analyzed the total amount of energy used in the all-laser procedure compared with traditional phacoemulsification and demonstrated lower levels of energy in the all-laser surgery compared with the use of ultrasound.13
Our group performed a study comparing three groups of patients undergoing cataract surgery (unpublished data). One group of 10 eyes underwent surgery with no femtosecond laser but with nanosecond laser (manual + nano group), a second set of 10 eyes underwent surgery with both the femtosecond laser and nanosecond laser (femto + nano group), and a third group of 10 eyes was treated with femtosecond laser and phacoemulsification (femto + phaco group). In these three groups, we compared the loss of endothelial cells and central corneal thickness 7 and 30 days after surgery. All patients included in the study had grade 3 cataracts.
In the manual + nano and femto + nano groups, less loss of endothelial cells and less corneal edema were seen compared with the femto + phaco group (Figures 2 and 3). Eyes in the femto + nano group required about 60% less energy compared with those in the manual + nano group (255 ± 75 mJ vs 833 ± 86 mJ; P = .0001).
Overall, performing surgery with the nanosecond laser system was simple, with a fast learning curve and no intraoperative complications.
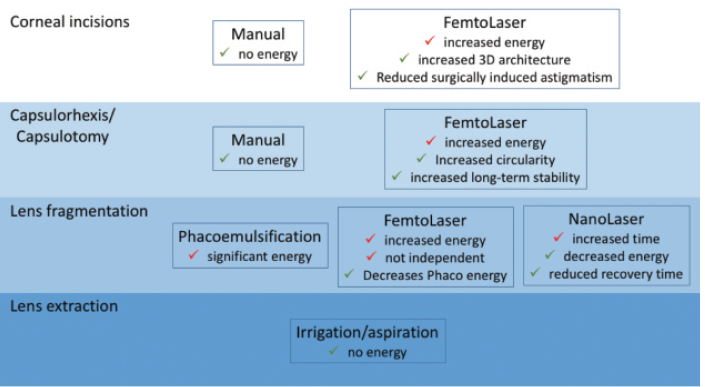
Figure 4. Pros and cons of the femtosecond laser, nanosecond laser, and conventional surgery.
CONCLUSION
Studies in the literature and our own clinical experience show that the nanosecond laser can improve the results of cataract surgery by reducing tissue trauma compared with surgery using ultrasound only. The all-laser combination of femtosecond laser and nanosecond laser for cataract surgery optimizes surgery by combining two sets of advantages: those of LACS in terms of better visual performance achieved by improving the capsulotomy and corneal incisions and those related to the reduced tissue trauma achieved by reducing ultrasound energy with the use of the nanosecond laser (Figure 4).
1. He L, Sheehyb K, Culbertson W. Femtosecond laser-assisted cataract surgery. Curr Opin Ophthalmol. 2011;22:43-52.
2. Alió JL, Abdou AA, Puente AA, Zato MA, Nagy Z. Femtosecond laser cataract surgery: updates on technologies and outcomes. J Refract Surg. 2014;30:420-427.
3. Mastropasqua L, Toto L, Mastropasqua A, et al. Femtosecond laser versus manual clear corneal incision in cataract surgery. J Refract Surg. 2014;30:27-33.
4. Masket S. Is there a relationship between clear corneal cataract incisions and endophthalmitis? J Cataract Refract Surg. 2005;31(4):643-645.
5. Nagy ZZ, Mastropasqua L, Knorz MC. The use of femtosecond lasers in cataract surgery: review of the published results with the LenSx system. J Refract Surg. 2014;30:730-740.
6. Mastropasqua L, Toto L, Mattei PA, et al. Optical coherence tomography and 3-dimensional confocal structured imaging system-guided femtosecond laser capsulotomy versus manual continuous curvilinear capsulorhexis. J Cataract Refract Surg. 2014;40(12):2035-2043.
7. Toto L, Calienno R, Curcio C, et al. Induced inflammation and apoptosis in femtosecond laser-assisted capsulotomies and manual capsulorhexes: an immunohistochemical study. J Refract Surg. 2015;31:290-294.
8. Mayer WJ, Klaproth OK, Hengerer FH, et al. In vitro immunohistochemical and morphological observations of penetrating corneal incisions created by a femtosecond laser used for assisted intraocular lens surgery. J Cataract Refract Surg. 2014;40:632-638.
9. Schultz T, Joachim SC, Stellbogen M, Dick HB. Prostaglandin release during femtosecond laser-assisted cataract surgery: main inducer. J Refract Surg. 2015;31:78-81.
10. Conrad-Hengerer I, Al Jubury M, Schultz T, MD, Hengerer FH, Dick HB. Corneal endothelial cell loss and corneal thickness in conventional compared with femtosecond laser-assisted cataract surgery: three-month follow-up. J Cataract Refract Surg. 2013;39:1307-1313.
11. Mayer WJ, Klaproth OK , Hengerer FH, Kohnen T. Impact of crystalline lens opacification on effective phacoemulsification time in femtosecond laser-assisted cataract surgery. Am J Ophthalmol. 2014;157:426-432.
12. Kanellopoulos AJ, Photolysis Investigative Group. Laser cataract surgery: a prospective clinical evaluation of 1000 consecutive laser cataract procedures using the Dodick photolysis Nd:YAG system. Ophthalmology. 2001;108(4):649-655.
13. Kanellopoulos AJ. All-laser bladeless cataract surgery, combining femtosecond and nanosecond lasers: a novel surgical technique. Clin Ophthalmol. 2013;7:1791-1795.
Leonardo Mastropasqua, MD
• Director, Ophthalmology Clinic, Department of Medicine and Science of Aging, University G. d’Annunzio of Chieti and Pescara, Italy
• National High Tech Center and National School of Robotic Surgery in Ophthalmology
• mastropa@unich.it
• Financial disclosure: None
P.A. Mattei, MD, PhD
• Senior resident in Ophthalmology, University G. d’Annunzio of Chieti and Pescara, Italy
• National High Tech Center and National School of Robotic Surgery in Ophthalmology
• pamattei@unich.it
• Financial disclosure: None
Lisa Toto, MD, PhD
• Researcher, Ophthalmology Clinic, Regional Center of Excellence in Ophthalmology, University G. D’Annunzio of Chieti and Pescara, Italy
• National High Tech Center and National School of Robotic Surgery in Ophthalmology • l.toto@unich.it
• Financial disclosure: None
