


Getting to Know You
Currently, what book are you reading, what TV series are you binge-watching, what app do you use the most, and where do you get your daily news?
Book: Try Hard! by Althaus Marcel.
TV series: Three German language series: Vorstadtweiber, München 7, and Tatort.
App: n-TV (news-TV).
News: n-TV, Focus Online, and the New York Times website and news apps.
What is something in your life you would happily do again, and what is something you would never do again?
Happily do again: Competitive sailing with the Tornado catamaran as a member of the German Olympic team in 1980. A picture of the catamaran, called the Flying Phantom, can be seen on page 66; STAAR Surgical has sponsored some of the catamaran’s technical equipment. My sons—one of whom is an ophthalmologist—is the only German team to qualify for the extreme sailing series: https://www.facebook.com/extremesailingseries/videos/1996004097092078/.
Never do again: Go to school.
What are three places at the top of your bucket list?
No. 1: Two holy sites: Dionysiou Monastery on Mount Athos, Greece, and the Potala Palace in Lhasa, Tibet, the residence of the Dalai Lama until he fled to India in 1959.
No. 2: The Way of St. James (the Camino de Santiago), the pilgrimage to Santiago de Compostela, Spain.
No. 3: Walking through the Alps from Munich to Venice, Italy, in 32 days.
If you had to donate half your income tomorrow, to whom would you give it?
I would donate to a number of nonprofit organizations in my local area as well as to Survival International, Médecins Sans Frontière (Doctors Without Borders), Welthungerhilfe, Amnesty International, and the World Wildlife Fund.
If there is one high-risk thing that you have not done but remain curious about, what is it?
Hang-gliding. (My beloved wife put a ban on it.)

Your Thoughts on Ophthalmology
What is the health care landscape like in your country?
In Germany, the health system is a little too complicated with too much bureaucracy. Nevertheless, we can live with it at the moment. Expectations for the future are quite sad.
How enthusiastic are you about the future of ophthalmology?
I am very enthusiastic. Ophthalmology is a highly innovative medical discipline. Many promising diagnostic and therapeutic tools are in the pipeline to help patients restore or keep their vision.
What products in the pipeline excite you most?
Products in development that hold the most interest for me include new accommodating IOLs, IOLs that are adjustable postoperatively via laser or light treatment, chips for restoring or replacing the function of retinal photoreceptors, and artificial cornea materials.
What was your most memorable moment in surgery?
An untreatable expulsive subchoroidal hemorrhage in an only eye.
What recent studies or technologies have influenced your surgical technique?
The femtosecond laser has quickly established an important place for itself in ophthalmic surgery. It provides unbeatable precision in corneal surgery, such as for flap or pocket creation for LASIK or SMILE, for creation of limbal relaxing incisions, and for performing penetrating or deep lamellar corneal transplantation. In advanced cataract surgery, it facilitates creation of capsulotomies centered on the lens apex. In my hands, femtosecond laser technology is mandatory for implanting diffractive multifocal and extended depth of focus IOLs, and for capsule-fixated IOLs such as the Bag in the Lens IOL (Morcher) and the Masket ND IOL (Morcher) for avoiding negative dysphotopsia.
What was the toughest decision you have had to make as an ophthalmologist?
To remove the second eyeball of a patient due to untreatable pain after a traffic accident.
How has ophthalmology changed since you started practicing?
Ophthalmology has changed in so many ways in the past 30 years. Consider the diagnostic workup. When I started practicing ophthalmology, we had the basic tools: medical history, visual acuity test, slit-lamp examination, funduscopy, and Goldmann visual field test. Today, things have changed in an amazing way, and computer technology is everywhere. I have been using electronic medical records for 20 years. Most modern diagnostic tools depend on a computer to work: OCT, biometry, topography, endothelial cell count, visual field testing, and many other technologies.
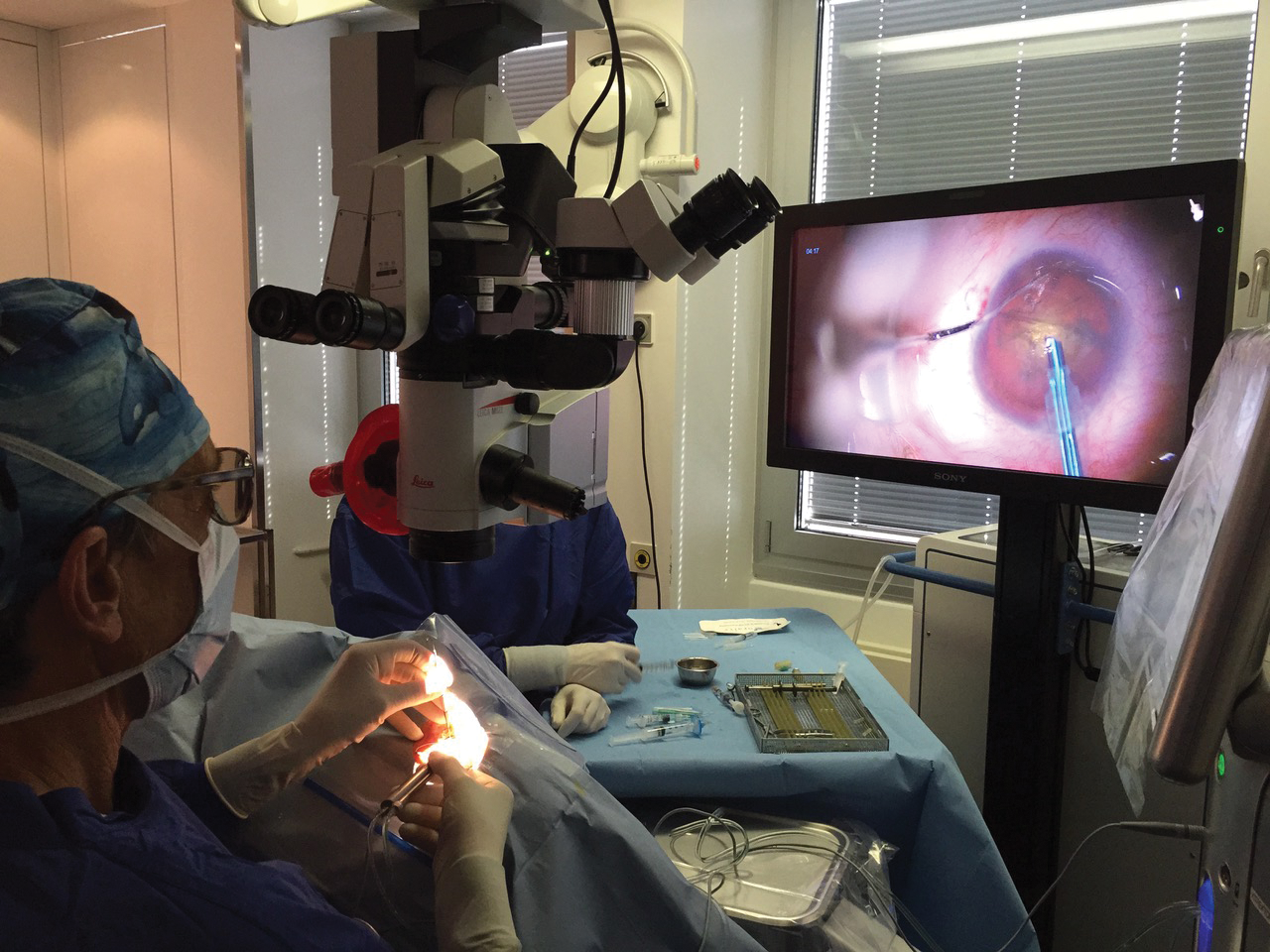
Again going back to when I started, cataract surgery was done with a loupe for magnification, with the surgeon in standing position, ungloved, using a Graefe knife. Intracapsular cataract extraction (which was super-easy in eyes with pseudoexfoliation syndrome) required a long corneal incision with both eyes patched for 1 week postoperatively. Innovations at that time—each one requiring a long and very emotional discussion—included using a surgical microscope, sewing the incision, wearing gloves, and patching only the operated eye. All cataract surgery was done as inpatient surgery with general anesthesia. Today, we operate with topical anesthesia, multifocal IOL implantation is common, and the patient goes home without a patch and with instant visual rehabilitation. Of course, with the innovation of heads-up surgical display, we can now operate in 3-D, again without looking through the microscope. What a change!
What advice can you offer the new generation of ophthalmologists?
Learn to use the basic diagnostic tools: taking a full and accurate medical history, performing a thorough slit-lamp examination, and performing funduscopy.
If you could trade lives with a fellow ophthalmologist for 1 day, who would it be and why?
I am happy as I am, thanks.
If you were forced to limit your practice of ophthalmology to one procedure, what procedure would you choose and why?
I would choose EVO Visian ICL (STAAR Surgical) implantation, performed with 3-D heads-up surgery. This is an aesthetically pleasing surgery that preserves the most powerful tissue of the human eye—the lens—for future procedures such as cataract surgery. Since 1999, we have had the Visian Toric ICL, so 96% of refractive disorders can be treated with the ICL. This posterior chamber phakic IOL is removable and/or exchangeable if newer lenses are developed (such as presbyopia correction with extended depth of focus, as most recently available with the EVO+ Visian ICL with Aspheric Optic). No lines of vision are lost, and patients are very happy postoperatively.


Your Thoughts on Business
What differentiates your practice from those of your competitors?
We offer the complete diagnostic and surgical ophthalmic spectrum for all patients, whether public insured, private insured, or refugees.
How do you feel about private equity, and is there a place for it in ophthalmology?
It is great for the retiring ophthalmologist because he or she can sell the practice immediately. It is difficult for the young self-employed ophthalmologist. Time will tell.
How do you approach marketing your practice and specific procedures you offer?
I use the tools that are allowed here in Germany: a web page; a social media presence on Facebook, LinkedIn, and Twitter; and Google ads.
How do you or your practice keep staff members happy?
This is the toughest question; we try hard every day to understand the needs of our employees. Every 4 weeks, we meet together and discuss what has gone well and what has gone wrong. Twice a year, we hire specialists to help staff members learn how to deal with and talk to complaining patients.
What is your end game?
I have no strict plan, but I certainly do not see myself working to age 80!
