



Dry eye, also referred to as dry eye disease (DED), is a common ocular complaint. Estimates of the prevalence of dry eye vary depending on how the disease is defined and diagnosed and on what population is under study: reports range from 7% prevalence in the United States to 33% in Taiwan and Japan.1 The condition affects older people more than younger and women more than men. Epidemiologic data from the large-scale, long-term Women’s Health Study and Physician’s Health Study indicate that the prevalence of symptomatic dry eye in US women and men over age 50 years is 7% and 4%, respectively.1-3
Eyes can feel dry for many reasons—among them, environmental conditions, allergies, and dysfunction on the ocular surface. Ocular surface problems can include insufficient tear production, goblet cell deficiency, and meibomian gland dysfunction (MGD), each leading in its own way to disruption of the delicate balance among the aqueous, mucous, and lipid components of the tear film. It was a decade ago that the International Dry Eye Workshop produced the following definition, which revolutionized the idea of DED: “Dry eye is a multifactorial disease of the tears and ocular surface that results in symptoms of discomfort, visual disturbance, and tear film instability with potential damage to the ocular surface. It is accompanied by increased osmolarity of the tear film and inflammation of the ocular surface.”4
When patients present with a complaint of dry eye, therefore, our first job is to figure out what kind of dry eye they have. I always have a candid conversation with my patients about certain people being more predisposed to dry eye. Women over 40, in particular, have normal hormonal changes that make dry eye more common. Some patients may have an underlying inflammatory condition as the cause, including autoimmune conditions such as Sjögren syndrome and rheumatoid arthritis. Dryness can be caused by a systemic medication that the individual is taking. Other reasons for ocular discomfort can include ectropion, entropion, or floppy eyelid syndrome, which must be distinguished from true dry eye. Allergy can also play a role.
Only then—when we have determined whether they have aqueous-deficient dry eye, MGD, environmental exacerbation, or some other cause of discomfort—can we find the correct solution to their problem. Although it is presented here as a clear-cut reason causing the dry eye, often it is a combination of several ultimately causing the signs and symptoms that we see.
While we are in the process of determining the cause, we have an ideal opportunity to educate our patients about the nature of their specific complaints and to explain why we will recommend a specific therapy or therapies to address their condition.
SHOWING THE CAUSE
A picture is worth a thousand words. As the examination of the patient with dry eye proceeds, we take pictures and videos to document our findings thoroughly. This allows us to show patients what is happening on the surface of their eyes and contrast that with pictures or videos from our library showing normal function. By doing this, we can tie the symptoms the patient is experiencing to a specific cause, so that we can then engage the patient in eliminating that cause. In the two cases below, pictures and videos allow the patient to visualize what we want to aim for with our suggested therapy: a healthier ocular surface.
Anterior blepharitis. For patients with anterior blepharitis, for example, we show them what their inflamed eyelids look like (Figure 1). We explain that those visible, crusty deposits must be washed off with a cleaning regimen to improve the health of their lids.
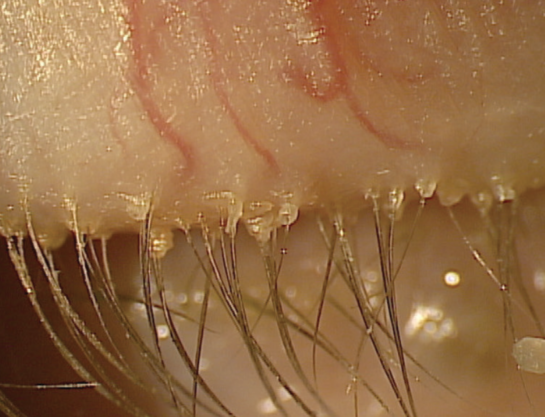
Figure 1. Presentation of blepharitis.
MGD. When MGD is present and the patient’s meibum is expressed as a paste, we can capture it on video (Figure 2) and compare it with a healthy eye, showing that the gland secretion should be thinner, more like an oil that lubricates the ocular surface.

Figure 2. Presentation of Meibomian gland dysfunction.
OTHER VISUAL AIDS and TACTICS
Plastic eye model. BlephEx, the maker of the BlephEx in-office treatment for dry eye and blepharitis, provides practitioners with a plastic model of the eyelid that can be used to demonstrate the anatomy to patients (Figure 3). This helps patients with blepharitis and other conditions to visualize the lids in 3-D, which then helps them direct their lid hygiene efforts properly.
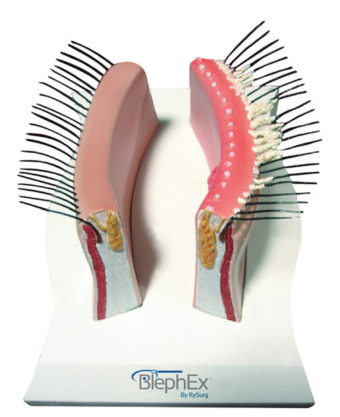
Figure 3. A plastic model of the eyelid.
Educational software. Rendia (formerly Eyemaginations) offers an educational suite that includes an illustrated depiction of the surface of the eye and videos showing, for example, how tears are produced and where they drain (Figure 4). If we are discussing punctal occlusion as being an appropriate treatment for a patient, he or she can form a clear picture of what that means and what the plugs will actually do in their eyes.
Figure 4. Patient education video explaining the role of tears in dry eye disease and the various tests available to diagnose it.
Product demonstration and coupon cards. Another thing that may seem minor but that we find helpful for patients is having sample bottles of prescription medications on hand—not necessarily to give out to patients, but rather to show them what the packaging looks like and how to dispense the drops. For example, Restasis Multidose (cyclosporine ophthalmic emulsion 0.05%; Allergan), introduced this past year, is the same preservative-free formulation as is present in the unit dose vials, but in a new dispenser with a one-way valve that prevents contamination of the bottle’s contents. It looks different from most topical drop bottles, and it might be daunting to a new user or to someone who is used to the old unit-dose packaging. Similarly, for nonpreserved single-use vials, we can show patients how to open the vial and apply the drops. Having those samples available to demonstrate in the examination room is quite helpful.
We also make sure to have coupon cards on hand for all the prescription medications we prescribe. This helps us emphasize to patients that this is a prescription medication, and they will simply not be able to find it over-the-counter; they must go to the pharmacist to get the prescription filled. It also demonstrates that we are dedicated to doing everything possible to make the medication affordable to them. We hope that it also improves compliance, as the cost of acquiring medications is one of the barriers decreasing compliance to the prescribed medication.
Question No. 1: What is causing my dry eyes?
Dr. Brujic: Although the cause is different for every patient, the examination we will perform today on your eyes is key to determining the reasons in your case. The most common causes, however, are that your eye is not making enough tears or is not lubricating your ocular surface sufficiently.
Google hit No. 2: Sometimes, there is a lack of balance in your tear-flow system. Or your air conditioner, heater, or other things around you could dry out your tear film. Other causes include:
The natural aging process, especially menopause
• Side effects of certain drugs like antihistamines
• Diseases that affect your ability to make tears, like Sjogren’s syndrome, rheumatoid arthritis, and collagen vascular diseases
• Problems that don’t allow your eyelids to close the way they should.1
1. http://www.webmd.com/eye-health/eye-health-dry-eyes#1
Question No. 2: Will I have to take these drops forever?
Dr. Brujic: As of right now, we really do not have any short-term fix for dry eye. We have long-term management options, and this drop is one of those options.
Google hit No. 3: Use artificial tears, gels, gel inserts, and ointments—available over the counter—as the first line of therapy. They offer temporary relief and provide an important replacement of naturally produced tears in patients with aqueous tear deficiency. Avoid artificial tears with preservatives if you need to apply them more than four times a day or preparations with chemicals that cause blood vessels to constrict.1
1. https://nei.nih.gov/health/dryeye/dryeye
Question No. 3: How frequently do you need to monitor me for this condition?
Dr. Brujic: I will see you back approximately 6 to 8 weeks after we have changed anything in your routine. Changing, in this instance, means either starting a therapy for a new dry eye patient or changing your therapeutic regimen. The 6-to-8-week interval allows us to determine how well the new treatment is working for you. If things are improving after that first follow-up, then I typically will see you again 3 months after that, to make sure that resolution of the signs and/or symptoms is sustained. Thereafter, you will need to come back every 6 months. As long as your signs and symptoms are somewhat well controlled, we will alternate your yearly vision checkup with a dry eye follow-up in between.
Google hit No. 7: See your doctor if you’ve had prolonged signs and symptoms of dry eyes, including red, irritated, tired, or painful eyes. Your doctor can take steps to determine what’s bothering your eyes or refer you to a specialist.1
1. http://www.mayoclinic.org/diseases-conditions/dry-eyes/basics/symptoms/con-20024129
Question No. 4: Is there anything nonprescription that I could use to alleviate these signs and symptoms?
Dr. Brujic: Neutraceuticals is one way that you can manage your dry eye without prescriptions. Also, appropriate nutrition and hygiene is key to maintaining the health of your eyelids, in particular the meibomian glands, which is one cause of dry eye problems in many cases.
Google hit No. 4: Sometimes simply changing your lifestyle habits may be enough to help improve your dry eye symptoms. Here are some things you can try:
• Avoid exposure to allergens
• Avoid hot, windy, low-humidity, and high-altitude environments
• Get an adequate amount of sleep and drink plenty of water
• Quit smoking and or avoid being around tobacco smoke
• Limit the amount of time you spend on activities that reduce blinking (eg, watching TV, reading, or computer use)
• Adopt a diet rich in omega-3 fatty acids (fish and fish oils, canola oil, flax seeds and flax seed oil, walnuts and walnut oil); they may reduce the inflammation associated with dry eye disease.1
1. http://www.dryeyedisease.ca/what-can-i-do/
Question No. 5: How much is this medication going to cost?
Dr. Brujic: Costs are tremendously variable, and, like dry eye itself, multifactorial. We do have coupons available to you, which can help to reduce your cost of prescription medications. But there are other costs and savings to consider, such as the over-the-counter drops you have been using to alleviate your symptoms and the time and aggravation you have experienced in dealing with your symptoms, possibly missing work time or leisure activities because of your discomfort. So cost depends not just on the amount of currency you are spending, but also on how much value you put on saving time and energy. Additionally, much of the expense of prescription medications may be borne by your insurer. The same is true for certain in-office treatments, such as punctal occlusion.
Google hit No. 1: It can cost about $30 to $300 or more per month for prescription eye lubricant medication. … For example, Drugstore.com charges about $10 to $20 for preservative-free artificial tears. Drugstore.com charges about $35 for a bottle of brand-name FreshKote [Focus Laboratories] prescription eye lubricant. It charges about $300 for a 1-month supply of the brand-name prescription eye emulsion Restasis [Allergan], if applied twice a day. It also charges about $300 per month for the brand-name prescription eye lubricant insert, Lacrisert [Bausch + Lomb].1
1. http://health.costhelper.com/dry-eyes.html
CONCLUSION
The unfortunate reality is that DED is more prevalent than practitioners think. It is important for clinicians to establish some type of protocol to identify patients with dry eye. The sooner we can start curbing those signs and symptoms, the better chance we have of making the ocular surface healthy again. When we find these patients earlier, we can promote a wellness mindset in the practice and the patients we are caring for. Through early treatment and appropriate education about their condition, patients will reduce their chances of developing the moderate to severe dry eye symptoms that are often much more difficult to resolve.
We can do this by utilizing tools that we frequently already have in our offices, such as a good anterior segment camera to demonstrate what the patient’s eye looks like or an eye model to point out where a problem lies. If we incorporate this mindset and these tools into every encounter we have with each patient, we can often help to make visible things that are seemingly invisible and help patients maintain the health of their delicate ocular surface.
1. Gayton JL. Etiology, prevalence, and treatment of dry eye disease. Clin Ophthalmol. 2009;3:405-412.
2. Schaumberg DA, Sullivan DA, Buring JE, et al. Prevalence of dry eye syndrome among US women. Am J Ophthalmol. 2003;136:318-326.
3. Moss SE, Klein R, Klein BE. Prevalence of and risk factors for dry eye syndrome. Arch Ophthalmol. 2000;118:1264-1268.
4. International Dry Eye Workshop (DEWS). The definition and classification of dry eye disease: report of the Definition and Classification Subcommittee of the International Dry Eye Workshop. Ocul Surf. 2007;5:75-92.
