



Performing cataract surgery in patients who have undergone corneal refractive surgery can be challenging, as preoperative biometry is often unreliable due to the influence of the earlier surgery. This can lead to selection of the wrong IOL in these patients who are accustomed to glasses-free vision and tend to have high visual expectations. RxSight’s Light Adjustable Lens (RxLAL; Figure 1) may be the most predictable way to provide optimal visual outcomes for these patients, as the lens can be precisely optimized after its implantation if the desired refractive result is not achieved.
AT A GLANCE
• Performing cataract surgery in patients who have undergone corneal refractive surgery can be challenging, as preoperative biometry is often unreliable due to the influence of the earlier surgery.
• Instead of relying on keratometry values, prediction of effective IOL position, and various IOL formulas for eyes with altered corneas, it may be better to adjust the refraction postoperatively.
• With the RxLAL, up to three office-based adjustments, each taking approximately 90 seconds, can be made to fine-tune refractive outcomes.
THE LIGHT ADJUSTABLE LENS
The RxLAL is adjusted postoperatively with an office-based Light Delivery Device (LDD) that resembles a slit-lamp Nd:YAG laser. The LDD delivers a predetermined pattern and amount of UV-A light (365 nm wavelength) to the photosensitive silicone lens, inducing precise modifications in lens curvature based on principles of photochemistry and diffusion.
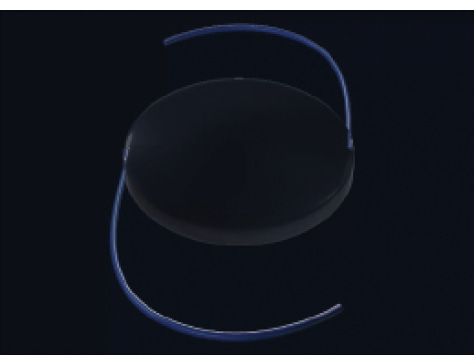
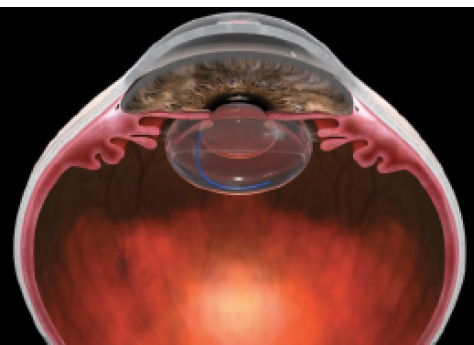
Figure 1. Illustrations show the three-piece design of the RxLAL (Above) and its position after implantation (Below).
The photosensitive lens incorporates proprietary silicone photoreactive additives called macromers, which are distributed throughout the lens. When light is directed to a specific area of the lens, macromers in the path of the light attach to the ends of other macromers, forming polymers. The remaining unreacted macromers physically diffuse into the exposed area, causing a highly predictable change in the curvature of the lens. As long as there are unpolymerized macromers, further adjustments to refine the refractive power can be made by applying light to different areas of the lens.
Utilizing a sub–3-mm clear corneal incision, the RxLAL is implanted like any standard foldable monofocal IOL. Its three-piece design features a 6-mm optic diameter and 13-mm overall length. After a period of postoperative refractive stabilization (approximately 2 weeks after surgery), the lens is adjusted noninvasively. Postoperative adjustments can range from -2.00 to 2.00 D sphere and from 0.50 to 3.00 D cylinder in any combination.
Up to three office-based adjustments, each taking approximately 90 seconds, can be made to fine-tune refractive outcomes. Once the patient’s vision is optimal, the IOL is permanently locked in at its current refractive state, preventing further power changes. The RxLAL is sensitive to UV-A light until the adjustment process is completed, so, until final lock-in, patients must wear UV-protective glasses to avoid incidental exposure from sunlight.
A prospective, nonrandomized clinical trial including 122 previously unoperated eyes of 91 patients with significant cataract (virgin eyes) was conducted at the Center for Vision Science, Ruhr University Eye Clinic, in Bochum, Germany. Postoperatively, 98% of eyes were within 0.50 D of target manifest refraction spherical equivalent (MRSE), 100% had UCVA of 20/25 or better, and 88% had UCVA of 20/20 or better.1
John F. Doane, MD, a clinical investigator in the pivotal study for US FDA approval of the lens, shared similar study outcomes at the 2017 American-European Congress of Ophthalmic Surgery (AECOS) Winter Symposium in Aspen, Colorado. In that study, more than 90% of 391 RxLAL eyes were within 0.50 D of target MRSE, 92% had a UCVA of 20/25 or better, and more than 70% had a UCVA of 20/20 or better. In both studies, nearly 30% of eyes had a UCVA of 20/16 or better.2
By comparison, in a recently published meta-analysis of toric IOLs,3 only 65% of eyes achieved 20/25 or better postoperative UCVA.
AFTER CORNEAL REFRACTIVE SURGERY
Postoperative adjustability clearly reduces the degree of error from imprecision in biometry, power calculation, and postimplantation movement of the IOL. However, this problem becomes even more challenging in eyes that have undergone previous LASIK, PRK, or another corneal refractive surgical procedure, due to additional abnormalities from irregular corneal surfaces.
LASIK is the most common refractive surgical procedure in ophthalmology today, and many who have undergone the procedure are now reaching cataract surgery age. The RxLAL may, therefore, present a superior approach for achieving desired outcomes of cataract surgery in these post-LASIK eyes. Instead of relying on keratometry values, prediction of effective IOL position, and various IOL formulas for eyes with altered corneas, it may be better to simply adjust the refraction postoperatively. This would reduce the burden of having to achieve emmetropia immediately after surgery in these complicated cases.
Results with the RxLAL in postrefractive surgery eyes have been published, most notably by Brierley.4 In this retrospective study of 34 postrefractive surgery eyes in 21 patients, the MRSE relative to target refraction after final lock-in with the RxLAL was within ±0.25 D in 74% of eyes, ±0.50 D in 97% of eyes, and ±1.00 D in 100% of eyes. These results were 60% more predictable than the best refractive outcomes achieved in previous studies with monofocal IOLs in postrefractive surgery eyes.4
When I practiced at Ruhr University Eye Clinic, I participated in a multicenter, international, collaborative analysis to better understand the clinical results in postrefractive surgery eyes implanted with the RxLAL. This retrospective analysis, performed by four surgeons in three countries, included 37 eyes with a history of at least one corneal refractive procedure (LASIK, PRK, RK, or CK) prior to RxLAL implantation. Twenty eyes were targeted for distance (emmetropia) and 17 for near vision (adjustable monovision).
Analysis of the distance-corrected eyes (n=20) showed that 70% of eyes achieved a postadjustment UDVA of 20/25 or better, with an overall improvement from preadjustment UDVA to postadjustment UDVA of more than 2 lines. Only 40% of eyes were within ±0.50 D MRSE before adjustment, but this improved to 95% (19 of 20) after the lens was adjusted and locked in. The postadjustment MRSE showed a marked improvement over published results with the modified Masket method, in which 67% of previous LASIK and PRK patients were reported within ±0.50 D of target MRSE.5
Seventeen eyes in this analysis were targeted for near vision (adjustable monovision), with a mean target refractive goal of -1.50 D. After adjustment and lock-in, the average MRSE was -1.50 ±0.55 D, and average UNVA was 20/25 (J2), demonstrating that near vision eyes implanted with the RxLAL can be adjusted to achieve the proper amount of desired myopia.
CONCLUSION
In my experience, the RxLAL is an effective and promising option for avoiding the inaccurate biometry readings and managing refractive surprises that are often seen after IOL implantation in postrefractive surgery eyes. Due to its postoperative adjustability, the RxLAL offers a level of refractive precision superior to that of nonadjustable IOLs. Additionally, this group of patients that has previoulsy undergone refractive surgery understands the value of excellent uncorrected vision and is generally willing to pay for a superior outcome.
Other benefits of the RxLAL include improved binocular accuracy with monovision treatments. Although monovision is a common strategy used to address presbyopia, the surgeon’s ability to achieve the desired offset and patient tolerance can be highly unpredictable. With the RxLAL, not only is the surgeon able to offer a more accurate visual outcome, but also the patient can preview the outcome, the surgeon can then adjust the monovision offset as desired.
1. Hengerer F, Dick B, Conrad-Hengerer I. Clinical evaluation of ultraviolet light adjustable intraocular lens implanted after cataract removal. Ophthalmology. 2011;118:2382-2388.
2. Doane J. Prediction to prescription—the future of cataract surgery. Paper presented at: the American-European Congress of Ophthalmic Surgery. February 26-March 1, 2017; Aspen, Colorado.
3. Kessel L, Andresen J, Tendal B, Erngaard D, Flesner P, Hjortdal J. Toric intraocular lenses in the correction of astigmatism during cataract surgery – a systematic review and meta-analysis. Ophthalmology. 2016;123:275-286.
4. Brierley L. Refractive results after implantation of a light-adjustable intraocular lens in postrefractive surgery cataract patients. Ophthalmology. 2013;120:1968-1972.
5. Wang L, Hill W, Koch D. Evaluation of intraocular lens power prediction methods using the American Society of Cataract and Refractive Surgeons post-keratorefractive intraocular lens power calculator. J Cataract Refract Surg. 2010;36:1466-1473.
