


By definition, a therapeutic lens or bandage lens is a contact lens that protects and heals the cornea. In this sense, nearly every type of contact lens can be used in a therapeutic capacity, and conditions recalcitrant to other treatment modalities may heal more readily with the use of a therapeutic contact lens.
Therapeutic contact lenses offer several advantages for patients who have undergone refractive surgery. The most widely used application is for bandage purposes immediately after surgery, when the primary aims are to:
• Protect the loosely adherent and regenerating epithelium from the action of the eyelids during healing;
• Aid the regeneration processes of the cornea;
• Assist in the regeneration of basement membrane and restoration of tight epithelial stromal adhesion;
• Provide pain relief and comfort; and
• Reduce inflammatory cell infiltration into the corneal stroma, decreasing the threat of corneal scarring.

SOFT LENSES ARE MAINLY USED FOR BANDAGE PURPOSES AFTER REFRACTIVE SURGERY
In the soft lens category, there are disposable hydrogel contact lenses and the relatively newer hyper–oxygen-permeable materials, the silicone hydrogels.
AT A GLANCE
• A therapeutic lens or bandage lens is a contact lens that protects and heals the cornea.
• After refractive surgery, soft contact lenses can be used to promote reepithelialization, control discomfort, reduce inflammatory reaction, and decrease the risk of corneal scarring.
• Use of silicone hydrogel lenses made of high Dk materials seems to be the best choice.
Successful wear of a bandage lens is dependent on the material and surface properties of the lens. Because bandage lenses are used overnight, they must allow sufficient oxygen flow to the cornea in order to maintain corneal aerobic metabolism. This is particularly important in a healing cornea with compromised epithelium. Studies have shown that a minimum oxygen transmissibility value of 87x10-9 units is required to avoid lens-induced corneal edema1 and of 125x10-9 units to avoid stromal anoxia.2
Conventional hydrogel contact lenses made of crosslinked hydrophilic polymers and water rely on the water to carry oxygen through the lens. This has been a limiting factor because, even if the lens is made up of 100% water, it can have an oxygen transmissibility (Dk) of only about 80x10-9 units. As a result, conventional hydrogel lens materials can have a Dk of at most 30 to 40x10-9 units, far below the limits for safe overnight wear. However, the silicone component of silicone hydrogel lenses provides extremely high oxygen permeability—five to six times that of conventional hydrogel lenses—without dependence on water content.
An additional requirement of bandage lenses is that mechanical trauma to the cornea should be minimal. Modulus or rigidity of the material can affect patient comfort, with less rigid lenses being more comfortable. Stiffer lenses may cause mechanical problems, and inadequate draping over the cornea by higher-modulus lenses may induce an abrasive shear force on the regenerating epithelium.
Lens surface properties such as wettability and deposit formation are important for stable vision, patient comfort, and biocompatibility. Surface smoothness and increased hydrophilicity result in better lens-surface lubrication and improved comfort.

HYDROGEL LENSES HAVE BEEN LARGELY REPLACED BY SILICONE HYDROGELS FOR THERAPEUTIC USE
Soft hydrogel lenses with moderate to high water content have been commonly used as bandage lenses after refractive surgery because of their comfort, ease of handling, and relatively high Dk. However, the high water content of these lenses makes them prone to drying. The dehydrated lenses become warped and often collect deposits that can increase the risk of infection and reduce patient comfort. As the lens draws water from the ocular surface and competes with the cornea for hydration, this can lead to corneal desiccation and staining.
Today, hydrogel lenses have been largely replaced by silicone hydrogels for therapeutic use. The advantages of silicone hydrogels include high oxygen transmission to promote healing and to prevent edema of the cornea or stromal flap during overnight wear. Lower water content makes these lenses more resistant to on-eye dehydration, and their nonionic surface attracts fewer protein deposits. Relative disadvantages such as stiffness, poor surface wettability, and lipid deposition have been minimized with newer-generation materials.
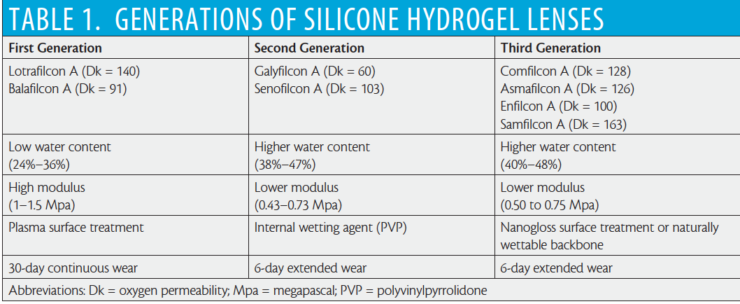
The pioneering first-generation silicone hydrogel lens materials, balafilcon A and lotrafilcon A, were introduced more than 15 years ago, and they continue to perform well. Lenses made with these materials have high Dk and low water content. First-generation silicone hydrogel lenses must undergo a surface treatment to hide the silicone from the tear layer and to make the lenses wettable. These lenses have a relatively high lens modulus, and issues such as discomfort and mechanical complications are possible with extended wear.
In 2004, intrinsically wettable second-generation silicone hydrogel materials were introduced. Lenses made with these materials have a lower modulus, related to their higher water content. Third-generation silicon hydrogels still show a decrease in modulus with higher water content, but they break the traditional inverse relationship between Dk and water content, exhibiting a higher Dk than water content (Table 1).

Silicone hydrogel lens models from three manufacturers are US FDA–approved for bandage use (Table 2). However, any silicone hydrogel lens can be used with success for bandage purposes.

ROUTINE USE OF BANDAGE CONTACT LENSES AFTER PRK, LASEK, OR EPI-LASIK IS WELL ACCEPTED
PRK, epi-LASIK, and LASEK are well-established, flapless refractive surgical procedures that are performed in about 20% of refractive surgery patients. Routine use of bandage contact lenses for 4 to 5 days after these surgeries is well accepted. This treatment was initially used to reduce postoperative pain and decrease dependence on pain medications. However, subsequent studies found that application of a bandage contact lens increased the rate and quality of epithelial wound healing and diminished corneal haze after PRK.
Although hydrogel lenses with mid to high water content have been most often used after refractive surgery, their Dk may lead to corneal swelling in overnight wear, which may diminish epithelial adhesion during healing; thus, their use has been mostly replaced by silicon hydrogel lenses. For bandage purposes, different types of silicone hydrogels lenses, from first to newest generation, have been used.3-10 Silicone hydrogel lenses have been reported to be superior to conventional hydrogels in achieving faster reepithelialization and reducing discomfort11 and in producing better postoperative results in terms of corneal haze and visual acuity at 1 month postoperative.12
Similar healing effects have been reported with different types of silicone hydrogel lenses, with complete reepithelialization achieved by day 4 or 5 postoperatively. Lower-modulus, newer-generation silicone hydrogel lenses may offer better comfort and faster epithelial healing compared with more rigid first-generation silicone hydrogel lenses.4-10

BANDAGE CONTACT LENS USE AFTER ROUTINE LASIK IS CONTROVERSIAL
Some authors advocate the use of bandage contact lenses for the first 2 days after LASIK to provide additional comfort,13 protect the flap, and prevent epithelial ingrowth.14 Some recommend short-term use, removing the lenses 1 hour after surgery, to control discomfort in the immediate postoperative period.15 Others claim that routine use of a bandage contact lens is not necessary in the postoperative LASIK patient.16-18
In interpreting these results, we must keep in mind that the lenses used in these studies were low Dk hydrogel lenses. Bandage contact lens use causes increased corneal and flap edema in the first postoperative day and, hence, decreases visual acuity.16,17 Compared with a bandage contact lens, topical NSAIDs and analgesics are more effective in relieving postoperative discomfort after LASIK.17 Routine use of a bandage contact lens does not prevent the occurrence of flap microstriae.18 Half of patients would prefer not to wear bandage contact lenses because of discomfort and blurred vision caused by the lenses.18
However, bandage contact lens use in the treatment of post-LASIK complications is well accepted. They are effective in treating epithelium-related complications, such as epithelial defects, recurrent epithelial erosions, and epithelial ingrowth,19-20 which occur more often in patients with anterior membrane dystrophies. They are also effective in treating flap-related complications, such as micro- and macrostriae.21-22

USE OF A BANDAGE LENS AFTER REFRACTIVE SURGERY IS NOT WITHOUT PROBLEMS
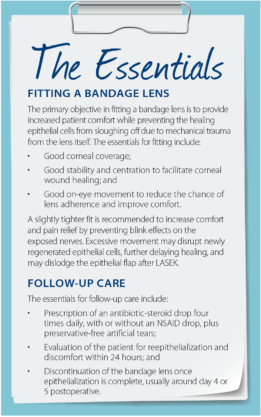
As with any contact lens patient, and more so in those with compromised corneas, proper fitting and follow-up care are essential to success with bandage lenses (see The Essentials). Nevertheless, the use of a bandage lens after refractive surgery is not without potential problems. Infectious keratitis is a rare but devastating complication after PRK or LASEK. Disruption of epithelial integrity introduces a potential risk factor for corneal infection. By providing a local environment suitable for infection, a bandage lens may further increase this risk. In a study of 12 cases of infectious keratitis after PRK, four had manual manipulation of the bandage lens as a risk factor.23
Despite the use of prophylactic antibiotics, bacteria can colonize bandage lenses, and the incidence of this is higher with LASEK than PRK.24,25 It is likely that devitalized cells on the epithelial flap, shed beneath the contact lens, provide a suitable environment for bacterial colonization. Colonizing bacteria are generally elements of the normal conjunctiva and eyelid flora.26
Sterile peripheral corneal infiltrates are a relatively benign complication of contact lens use. They are more common with extended wear, and the rate is higher with silicone hydrogel lenses.27 Infiltrative keratitis has also been shown to occur with therapeutic contact lens use after PRK.12 Sterile peripheral infiltrates are a self-limiting complication with full resolution after removal of the lens. Ocular lubricants may alleviate symptoms, and topical steroids may expedite resolution.
CONCLUSION
Soft contact lenses can be used as effective bandages after refractive surgery procedures, promoting reepithelialization, controlling discomfort, reducing inflammatory reaction, and decreasing the risk of corneal scarring. Considering the need for overnight wear in a damaged cornea with a compromised epithelium, use of silicone hydrogel lenses made of high Dk materials seems to be the best choice.
1. Holden BA, Mertz GW. Critical oxygen levels to avoid corneal edema for daily and extended wear contact lenses. Invest Ophthalmol Vis Sci. 1984;25:1161-1167.
2. Harvitt DM, Bonanno JA. Re-evaluation of the oxygen diffusion model for predicting minimum contact lens Dk/t values needed to avoid corneal anoxia. Optom Vis Sci. 1999;76:712-719.
3. Grentzelos MA, Plainis S, Astyrakakis NI, et al. Efficacy of 2 types of silicone hydrogel bandage contact lenses after photorefractive keratectomy. J Cataract Refract Surg. 2009;35:2103-2108.
4. Mohammadpour M, Amouzegar A, Hashemi H, et al. Comparison of lotrafilcon B and balafilcon A silicone hydrogel bandage contact lenses in reducing pain and discomfort after photorefractive keratectomy: a contralateral eye study. Cont Lens Anterior Eye. 2015;38:211-214.
5. Taylor KR, Caldwell MC, Payne AM, et al. Comparison of 3 silicone hydrogel bandage soft contact lenses for pain control after photorefractive keratectomy. J Cataract Refract Surg. 2014;40:1798-1804.
6. Gil-Cazorla R, Teus MA, Hernández-Verdejo JL, De Benito-Llopis L, García-González M. Comparative study of two silicone hydrogel contact lenses used as bandage contact lenses after LASEK. Optom Vis Sci. 2008;85:884-888.
7. Qu XM, Dai JH, Jiang ZY, Qian YF. Clinic study on silicone hydrogel contact lenses used as bandage contact lenses after LASEK surgery. Int J Ophthalmol. 2011;4:314-318.
8. Plaka A, Grentzelos MA, Astyrakakis NI, Kymionis GD, Pallikaris IG, Plainis S. Efficacy of two silicone-hydrogel contact lenses for bandage use after photorefractive keratectomy. Cont Lens Anterior Eye. 2013;36:243-246.
9. Mukherjee A, Ioannides A, Aslanides I. Comparative evaluation of comfilcon A and senofilcon A bandage contact lenses after transepithelial photorefractive keratectomy. J Optom. 2015;8:27-32.
10. Eliaçık M, Erdur SK, Gülkılık G, Özsütçü M, Karabela Y. Compare the effects of two silicone-hydrogel bandage contact lenses on epithelial healing after photorefractive keratectomy with anterior segment optical coherence tomography. Cont Lens Anterior Eye. 2015;38:215-219.
11. Engle AT, Laurent JM, Schallhorn SC, et al. Masked comparison of silicone hydrogel lotrafilcon A and etafilcon A extended-wear bandage contact lens wear after photorefractive keratectomy. J Cataract Refract Surg. 2005;31:681-686.
12. Edwards JD, Bower KS, Sedig DA, et al. Effects of lotrafilcon A and omafilcon A bandage contact lenses on visual outcomes after photorefractive surgery. J Cataract Refract Surg. 2008;34:1288-1294.
13. Mackool RJ. Bandage contact lens after LASIK. J Cataract Refract Surg. 2002;28:911-912.
14. Walker MB, Wilson SE. Incidence and prevention of epithelial growth within the interface after laser in situ keratomileusis. Cornea. 2000;19:170-173.
15. Orucov F, Frucht-Pery J, Raiskup FD, Strasman E, Landau D, Solomon A. Quantitative assessment of bandage soft contact lens wear immediately after LASIK. J Refract Surg. 2010;26:744-748.
16. Montes M, Chayet AS, Castellanos A, Robledo N. Use of bandage contact lenses after laser in situ keratomileusis. J Refract Surg. 1997;13(5 Suppl):S430-431.
17. Ahmed II, Breslin CW. Role of the bandage soft contact lens in the postoperative laser in situ keratomileusis patient. J Cataract Refract Surg. 2001;27:1932-1936.
18. Sekundo W, Dick HB, Meyer CH. Benefits and side effects of bandage soft contact lens application after LASIK: a prospective randomized study. Ophthalmology. 2005;112:2180-2183.
19. Oruçoglu F, Kendusim M, Ayoglu B, Toksu B, Goker S. Incidence and management of epithelial loosening after LASIK. Int Ophthalmol. 2012;32:225-228.
20. Asano-Kato N, Toda I, Hori-Komai Y, Takano Y, Tsubota K. Epithelial ingrowth after laser in situ keratomileusis: clinical features and possible mechanisms. Am J Ophthalmol. 2002;134:801-807.
21. von Kulajta P, Stark WJ, O’Brien TP. Management of flap striae. Int Ophthalmol Clin. 2000;40:87-92.
22. Pannu JS. Incidence and treatment of wrinkled corneal flap following LASIK. J Cataract Refract Surg. 1997;23:695-696.
23. Donnenfeld ED, O’Brien TP, Solomon R, Perry HD, Speaker MG, Wittpenn J. Infectious keratitis after photorefractive keratectomy. Ophthalmology. 2003;110:743-747.
24. Hondur A, Bilgihan K, Cirak MY, Dogan O, Erdinc A, Hasanreisoglu B. Microbiologic study of soft contact lenses after laser subepithelial keratectomy for myopia. Eye Contact Lens. 2008;34:24-27.
25. Liu X, Wang P, Kao AA, Jiang Y, Li Y, Long Q. Bacterial contaminants of bandage contact lenses used after laser subepithelial or photorefractive keratectomy. Eye Contact Lens. 2012;38:227-230.
26. Dantas PE, Nishiwaki-Dantas MC, Ojeda VH, Holzchuh N, Mimica LJ. Microbiological study of disposable soft contact lenses after photorefractive keratectomy. CLAO J. 2000;26(1):26-29.
27. Morgan PB, Efron N, Hill EA, Raynor MK, Whiting MA, Tullo AB. Incidence of keratitis of varying severity among contact lens wearers. Br J Ophthalmol. 2005;89(4):430-436.



