


QUESTIONS
1. What is your immediate reaction to the miLoop (IanTech)?
2. In your opinion, what is the potential of the product?
3. Would you consider using the miLoop when it becomes available? If you are skeptical, why wouldn’t you?
1. My immediate reaction was, “Why didn’t I think of this?” The miLoop is a simple device that can reduce the energy required to remove a cataract, and it can be done with a short learning curve.
2. I believe the miLoop could eliminate the need for phacoemulsification during cataract surgery. The removal of a cataract requires a certain amount of energy, and the bulk of that energy can be delivered with a femtosecond laser followed by minimal phacoemulsification or entirely with phacoemulsification. Both techniques always put energy into the eye, which requires recovery. With the miLoop, the cataract—no matter how hard—can be fragmented into smaller pieces without any energy. The miLoop also does not increase surgical time and could potentially even reduce surgical time.
3. I will definitely use the miLoop when it becomes commercially available. I have never thought of the phaco portion of cataract surgery as being a burdonsome step. However, when I used the miLoop in every other case on a 40-case day, I quickly wanted to use one every time because phacoemulsification seemed to be more of a burden. In short, I look forward to eliminating my phaco machine from the cataract surgery procedure. Also, outside the United States where modern phaco technology is not available, the miLoop will allow removal of the densest cataracts with little effort.

1. I was aware of the technology and had previously seen videos of the miLoop being used in cataract surgery. The device is essentially a modification of the lens snare, which has been used for many years in conjunction with small-incision sutureless extracapsular cataract extraction (Figure 1). The difference between the devices is that the loop of the miLoop is made of nitinol, which is an alloy that has memory—in this case, the shape of the lens nucleus. The loop is slipped around the nucleus in the bag to transect it.
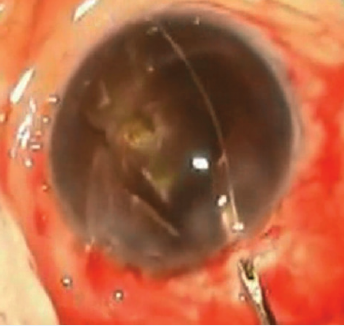
Figure 1. The nucleus is cut into three pieces with the lens snare. Each piece is then removed manually through a 4-mm incision with no ultrasound.
2. I think that there may be some use for the miLoop in very dense cataracts that are difficult to chop. The Akahoshi prechop technique and standard chopping both work well with medium nuclei. I suppose that very soft nuclei could be divided with the miLoop to facilitate removal; however, I would be concerned about damaging the edge of the capsulotomy if the opening were too small.
3. It would certainly be worth a try to see how easy the miLoop is to use in real life.

1. I have done about 30 cases with the miLoop in all types of cataracts, from very soft to very dense. My first impression was that it was much easier to do than I expected. I was easily able to get the injector through a sub–2-mm wound, and, after a few cases, I was able to perform nuclear cleaving in less than 1 minute. However, it does take some skill, concentration, and a steady hand to deliver the device under the capsular edge and open it with the trigger to extend the device around the nucleus. This must be achieved while maintaining the tip of the injector in the anterior capsular plane as you rotate your wrist clockwise. In other words, it is not a completely simple maneuver. For example, if the miLoop were delivered above the capsule in the sulcus space and rotated behind the capsule by accident, the consequences would be devastating.
2. There is a huge payoff with the miLoop, as it beautifully cracks even the densest cataracts in halves and quarters. As the loop is retracted into the injector, a dense nucleus will often tilt or prolapse, so it is helpful to have a second instrument in the eye to hold the nucleus down in the bag. In my opinion, the device is not super-helpful for soft cataracts, but I do feel it is an absolute game-changer for dense cataracts. It is important to do a good hydrodissection and ensure free nucleus rotation prior to using the device. I do not think the miLoop will replace phacoemulsification because ultrasound is still needed to remove the dense quadrants, but using the device can significantly reduce phaco energy and effective phaco time by allowing the surgeon to completely bypass the first sculpt and cracking phaco settings and proceed directly to a higher-vacuum quadrant removal setting.
3. I certainly plan on using the miLoop on dense cataracts, especially those in which laser fragmentation is not done. Sculpting with phacoemulsification and cracking extremely dense cataracts are two of the most challenging aspects of cataract surgery, and they are often the source of capsular tears. The device has the potential to greatly reduce this risk. In geographic and demographic pockets where dense rock hard cataracts are prevalent, this device is a must-have.

