



My Dear Colleagues,
I hope you all had an opportunity to read the cover focus, Going Places, in the April issue of CRST Europe. If you did, I know you enjoyed the insights of your colleagues from around the world regarding what they learned from their participation in international blindness prevention efforts, and how this knowledge in turn affected their practices in the developed world. It turns out that hard work, teamwork, a systematic approach to problem-solving, and innovative thinking are skills that provide benefits no matter where one hangs one’s hat.
AT A GLANCE
• Knowing manual excision techniques such as MSICS and ECCE can be helpful for complicated cases or when phacoemulsification might be too risky.
• Many of the skills for MSICS transfer directly over from phaco surgery, so the learning curve should not be steep.
In the issue, you also read comments from more than one contributor touting the value of being skilled with manual small-incision cataract surgery (MSICS). This approach to cataract removal uses a larger incision than phacoemulsification, yet large-scale comparative trials have found the results of both procedures to be basically equivalent.1-4 And, as David F. Chang, MD, pointed out in his article in the Going Places issue, “Lessons All Cataract Surgeons Can Learn From the Developing World,” MSICS may actually be the safer choice in eyes with mature cataracts.5
In MSICS, a long, scleral tunnel incision is made, wide enough to allow expression of the nucleus (Figure 1A–1C) and yet, when carefully constructed, still self-sealing (Figure 1D) and largely astigmatically neutral. In the presence of a hard cataract, MSICS avoids the potential corneal endothelial trauma associated with long phaco times, and it is also faster and less expensive to perform.
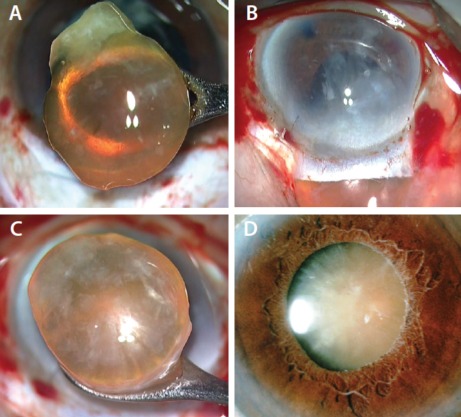
Figure 1. Manual excision of a cataract through a large incision (A–C). Preoperative photo of a mature cataract before MSICS (D).
Many surgeons, especially in the developed world, may think that they should perform only phacoemulsification cataract surgery. They cite phaco’s obvious advantages: The surgery requires only topical anesthesia; it uses a small incision and requires no sutures; and it provides clear uncorrected vision, usually by the day after surgery. But my opinion is that, just as there is more than one way to skin a cat, there is more than one way to remove a cataract. When young surgeons come to me for advice, I tell them that they should know a range of techniques, including phacoemulsification, MSICS, and extracapsular cataract extraction (ECCE). If you know it all, you can manage any type of cataract, in any type of patient, in any type of situation.
As Louis Pasteur said, “Fortune favors the prepared mind,” and, in our case, it favors the prepared hands of the surgeon.
WHY LEARN MSICS?
There are two main reasons why every cataract surgeon should be comfortable with MSICS.
Reason No. 1: It is helpful to be able to choose an alternative procedure when phacoemulsification looks too risky. When we are confronted with a hard brown or black cataract, we know that phacoemulsification of that rock-hard lens will be challenging for the surgeon—especially the novice surgeon—and potentially risky for the patient’s corneal endothelium. If the patient also has a low preoperative endothelial cell count, there is a risk of leaving the patient with bullous keratopathy, even if phacoemulsification proceeds without complication. In such cases, MSICS or ECCE would be a better choice.
Similarly, in very elderly patients (80+ years old), the capsular bag and the zonular apparatus may be weak. In such cases, which, again, are likely to involve a brown cataract, the chances of complications are increased, and MSICS would be a preferable choice to phacoemulsification.
Reason No. 2: It is helpful to be able to convert to MSICS in a complicated situation. When a complication occurs during phaco surgery, a little bit of postoperative residual astigmatism is preferable to a dropped nucleus. That is, if there is a rhexis extension and one has a choice between, on the one hand, continuing the phaco surgery and risking a more serious complication, or, on the other hand, converting to the safer MSICS procedure despite its slightly larger incision, the choice should be obvious. Knowing how to convert to MSICS in these situations is a must.
WHAT IS MSICS?
MSICS begins with a conjunctival peritomy, followed by creation of a long corneoscleral tunnel incision. A frown-shaped or straight incision of 6 to 7 mm width is made, and the tunnel is dissected in a flat plane, parallel to the floor, extending into clear cornea. A capsulorrhexis is created, followed by hydrodissection, and the nucleus is tilted or dialed into the anterior chamber.
A number of techniques can then be used to remove the nucleus through the scleral incision, including viscoexpression or use of a lens loop or irrigating vectis. Another strategy is to further divide the nucleus for easier removal, as with the miLoop device (IanTech), which cuts the nucleus into segments. (Editor’s Note: For more information on the miLoop, see Cataract Transection With a New Device, here.)
Cortex can then be removed with irrigation and aspiration and the IOL implanted in the intact capsular bag. At the close of surgery, the corneoscleral tunnel used for MSICS should be self-sealing and relatively astigmatically neutral.
MUTUALLY REINFORCING PROCEDURES
Note that many of the skills required for MSICS can be helpful to those who are learning phacoemulsification:
- All cataract surgeons should know how to create a scleral tunnel;
- All must learn to perform capsulorrhexis, as this is a vital step in phacoemulsification; and
- Hydrodissection is also key to phacoemulsification, as is cortical cleanup.
The only important difference is in nucleus removal, which is done manually in MSICS and with the ultrasound probe in phacoemulsification. Therefore, beginning surgeons can benefit from learning MSICS along with phacoemulsification, as so many of the skill sets for the two procedures are mutually reinforcing. Learning to do MSICS helps you be a better phaco surgeon, and vice versa.
CONVERTING TO MSICS
When a complication is encountered during phacoemulsification, sometimes the best option is to convert to MSICS. This is certainly the better course of action than dropping the nucleus and trying to chase it into the posterior chamber, which can lead to disaster. In this event, it is better to stop the phaco procedure and take a different tack.
The first and most important rule in converting from phacoemulsification to MSICS is this: Do not extend your clear corneal incision. Close the corneal phaco incision with a suture. Many surgeons use a temporal incision for phacoemulsification; if this is the case, move to a superior position and continue with a conjunctival peritomy.
If you were performing phacoemulsification under topical anesthesia, there is no need to perform a peribulbar or retrobulbar injection for a nerve block when you convert to MSICS. Instead, use what is called pinpoint anesthesia. Simply inject lidocaine subconjunctivally through a cannula on a syringe and deliver the drug near the insertion of the optic nerve; the patient will be comfortable. Then you can proceed to create the corneoscleral incision and complete the surgery as described earlier.
MSICS OR ECCE?
Sometimes the terms MSICS and ECCE are used interchangeably, but I make a distinction between the two. In MSICS, I perform capsulorrhexis and an incision of 6 to 7 mm. In ECCE, I make a slit capsulotomy and use a slightly bigger incision, perhaps 8 to 9 mm. Otherwise, the two procedures are similar.
When the patient’s zonules are very weak, that is the time to choose ECCE, as creating the capsulorrhexis for MSICS can apply tension on the zonules. Rather than risking zonular dialysis, it may be better to make a linear capsulotomy from about the 10- to the 2-o’clock position, and express the nucleus out through that slit. The IOL is then inserted through the same slit. This is sometimes referred to as the envelope technique. Once the IOL is in place, scissors can be used to complete the capsulotomy, leaving a clean opening in the anterior capsule.
The slightly larger ECCE incision will probably require a suture closure, in contrast to the usually sutureless MSICS incision.
CONCLUSION
I hope I have convinced you, my dear colleagues—especially my young colleagues, who may not have cut your teeth on ECCE, as many older surgeons did—that it is worth your time to acquire skill in MSICS. Think about it this way: It is better to have a tool in your toolbox that you may not need, rather than not to have it and find some day that you need it badly. As noted, many of the skills for MSICS transfer directly over from phaco surgery, so the learning curve should not be steep.
One last point I would like to mention is that some surgeons, perhaps more in the developing than the developed world, choose to do only MSICS. They say MSICS is better than phaco surgery, but I believe this is wrong. There is no doubt that the best technique for cataract removal is phacoemulsification. I say stick to phaco surgery for routine cases, but also learn MSICS and ECCE for when they may become necessary. If you have a nice, simple, uncomplicated cataract, please use phacoemulsification. But have the manual techniques in your pocket for situations such as those I have mentioned. They will stand you in good stead.
Respectfully,
1. Ruit S, Tabin G, Chang DF, et al. A prospective randomized clinical trial of phacoemulsification vs manual sutureless small incision extracapsular cataract surgery in Nepal. Am J Ophthalmol. 2007;143:32-38.
2. Venkatesh R, Chang DF, Muralikrishnan R , Hemal K, Gogate P, Sengupta S. Manual small incision cataract surgery: a review. Asia Pac J Ophthalmol (Phila). 2012;1(2):113-119.
3. Venkatesh R, Tan CS, Sengupta S, Ravindran RD, Krishnan KT, Chang DF. Phacoemulsification versus manual small-incision cataract surgery for white cataract. J Cataract Refract Surg. 2010;36:1849-1854.
4. Haripriya A, Chang DF, Reena M, Shekhar M. Analysis of complication rates of phacoemulsification and manual small-incision cataract surgery at Aravind Eye Hospital. J Cataract Refract Surg. 2012;38:1360-1369.
5. Chang DF. Lessons all cataract surgeons can learn from the developing world. CRST Europe. April 2017.MSICS transfer directly over from phaco surgery, so the learning curve should not be steep.
Amar Agarwal, MS, FRCS, FRCOphth
- Professor and Head, Dr. Agarwal’s Eye Hospital and Eye Research Centre, Chennai, India
- dragarwal@vsnl.com