

The intraocular maneuvers in cataract surgery occur entirely in the anterior chamber (AC), and therefore it is essential to maintain adequate AC depth throughout the surgical procedure. Having a shallow AC during phacoemulsification can be detrimental to the corneal endothelium and to other structures including iris tissue, the capsular bag, and the posterior capsule, which can increase the incidence of intraoperative complications. A pressurized infusion system is one of the most crucial elements to prevent surge and help to maintain AC depth.
When an occluded fragment is held at the phaco tip by high vacuum and then abruptly aspirated, fluid rushes into the phaco tip to equilibrate the built-up vacuum in the aspiration line, causing surge. This can in turn lead to shallowing or collapse of the AC. Various strategies are employed to combat surge, including the use of noncompliant tubing, small-bore aspiration line tubing, microflow tips, aspiration bypass systems, dual linear foot pedal control, and sophisticated microprocessors to sense fluctuations in the AC pressure.
In this surgical configuration, an automated air pump is used to push air into the infusion bottle, increasing the pressure with which the fluid flows into the eye. This increases the steady-state pressure of the eye, keeping the anterior chamber deep and well-maintained during the entire procedure. Use of this setup makes phacoemulsification a relatively safe procedure by reducing surge, even at high vacuum levels.
CAUSES OF SHALLOW AC
Modern phaco machines now have incorporated pressurized infusion systems that help to prevent AC shallowing to a great extent. Nevertheless, a shallow AC can occur due to other reasons, including inadequate inflow of fluid, excessive outflow of fluid, or positive posterior pressure. Specific causes may include the following:
Blockage of silicone sleeve: Too tight a corneal incision often constricts the silicone sleeve against the phaco tip. This hinders fluid inflow and may cause shallowing of the AC.
Leaking incision: A poorly constructed corneal incision that is wider than the bore of the phaco tip allows expulsion and leakage of fluid around its edges. This issue can be addressed by suturing the incision and creating a new one.
Increased vacuum: Mismatched parameters, with increased vacuum and low fluid infusion, tend to lead to the egress of more fluid from the eye than is entering the eye. This indirectly leads to shallow AC.
Small eyes: Pediatric and nanophthalmic eyes with short axial lengths have increased positive pressure. A vitreous tap can help relieve some of the pressure and consequently deepen the anterior chamber. Intravenous mannitol can be administered prophylactically to decrease the positive pressure and facilitate surgery.
Suprachoroidal effusion and hemorrhage also present a similar scenario, wherein it is essential to perform a vitreous tap to drain the fluid and/or blood. It is extremely important to understand that, in cases with suspected suprachoroidal hemorrhage, the corneal incision should not be enlarged. This can lead to more effusion and eventually culminate in an expulsive hemorrhage due to sudden lowering of the IOP.
Increased positive pressure can also occur due to a tight eyelid, in the event of excessive injection of an anesthetic agent into the lid. When this occurs, lateral canthotomy often helps to relieve the pressure.
TROCAR-ACM
For complicated surgeries, fluid infusion can be regulated with the help of an anterior chamber maintainer (ACM), a trocar-ACM combination,1,2 or a trocar placed in the pars plana.
The trocar-ACM is a novel concept that overcomes the shortcomings of standard ACMs. It does not require creation of a paracentesis incision matching the dimensions of the bore of an ACM. The trocar-ACM is introduced into the eye at a distance of 0.5 mm from the limbus, with care being taken that the needle enters the eye in front of the iris tissue. The trocar-ACM is introduced by creating a biplanar incision that is self-sealing. Its design and use are detailed in Figures 1 through 5.

Figure 1. The trocar-ACM assembly includes a trocar cannula and infusion tubing.

Figure 2. Magnified view of trocar-ACM shows the trocar blade with the cannula snugly fit onto it.
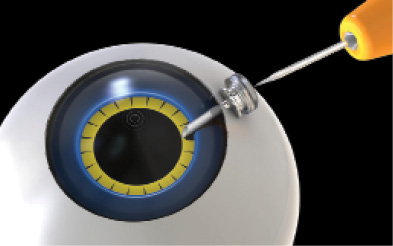
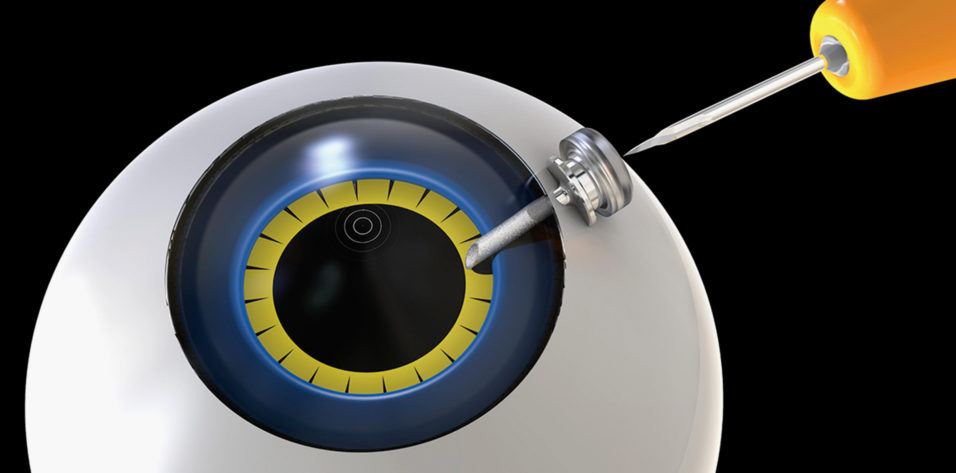
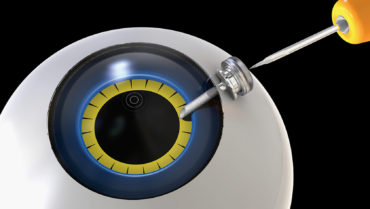
Figure 3. Illustration of trocar-ACM plugged in to the human eye. The trocar-ACM lies in front of the iris tissue.
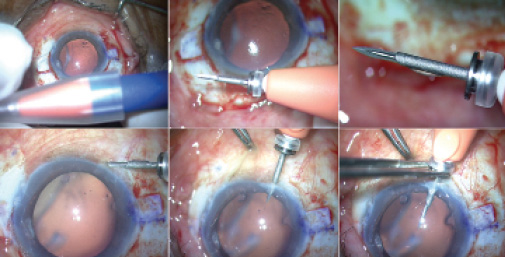
Figure 4. Clinical steps for placement of trocar-ACM. The trocar-ACM device with the cap on it (top left). The trocar-ACM device (top middle). Magnified view of the trocar blade and cannula (top right). Conjunctival displacement is done and trocar blade is placed at a distance of 0.5 mm from the limbus (bottom left). The trocar is introduced inside the eye so that the blade enters eye in front of the iris tissue (bottom middle). The hub of the cannula is flush with the surface of the sclera and held with forceps (bottom right).
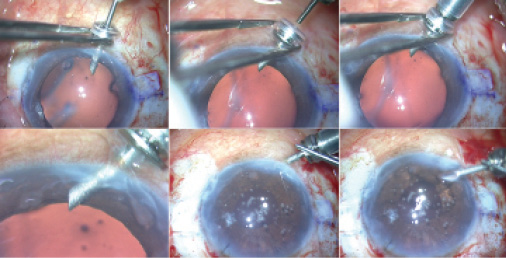
Figure 5. Clinical steps for placement of trocar-ACM, continued. While the cannula is held, the trocar blade is pulled out (top left). The infusion line is attached to the cannula hub (top middle and right). Placement of trocar-ACM in the anterior chamber (bottom left). After completion of surgery, the trocar-ACM is pulled out of the eye (bottom middle and right).
CONCLUSION
It is extremely important to maintain appropriate AC depth, and various methods can be employed to achieve this in order to optimize the outcomes of cataract surgery.
1. Narang P, Agarwal A, Kumar DA, Agarwal A, Agarwal A. Twenty-five-gauge trocar anterior chamber maintainer: new device for infusion. J Cataract Refract Surg. 2018;44(7):797-801.
2. Agarwal A, Narang P, Kumar DA, Agarwal A. Trocar anterior chamber maintainer: improvised infusion technique. J Cataract Refract Surg. 2016;42(2):185-189.
