




Innovations and refinement in techniques and technology have made cataract surgery one of the safest and most rewarding surgical procedures. But when mitotically active equatorial lens cells at the capsular fornices are left behind owing to imperfect cortical cleanup, preservation of the excellent visual results of cataract surgery are put in doubt. The posterior capsular opacification (PCO) that results from proliferation of lens epithelial cells (LECs) can hamper visual quality. LECs are the principal cause of clinical PCO.1 If these cells are left behind, no amount of anterior or posterior capsular polishing can prevent PCO formation.2,3
Despite this, cortical removal is one of the most neglected and underemphasized steps of phacoemulsification.4-6 In this article we describe tips for achieving safe and predictable cortical removal and how to deal with corticocapsular adhesions in cataract surgery.
CORTICAL ASPIRATION TECHNIQUE
Cortical cleaving hydrodissection is an important step in achieving thorough removal of the lens cortex and reducing PCO.7-9 This maneuver frees the cortex from the capsular fornices, thus making removal more effective. It also makes it safer by reducing stress on the capsulozonular complex.
A sign of a good cortical cleaving hydrodissection is the passage of a fluid wave across the posterior capsule. Care should be taken to tent up the anterior capsule a little prior to hydrodissection. This will help the fluid find a plane between the cortex and capsule, rather than create a hydrodelineation.
Irrigation and aspiration (I/A) for cortical removal can be performed using a bimanual or coaxial technique. The advantage of performing bimanual cortical aspiration is that, because there are two small valvular sideport incisions being used for cortex cleanup, a closed chamber is maintained at all times. There is minimal chance of leakage and subsequent shallowing of the anterior chamber.
Further, the biggest advantage for the surgeon is the ability to swap hands and perform thorough 360° cortex removal, including from the subincisional area. Often, during subincisional cortex removal with coaxial I/A, there is distortion at the main incision, which may lead to fluid leakage and/or leave clinically invisible incisional collagen damage that can affect wound healing.
Bimanual I/A also has the advantage that, if the surgeon is used to this technique in his or her routine cases, then performing bimanual maneuvers when needed—such as in the event of small pupils, floppy irides, or the need for anterior vitrectomy—is easy and familiar for the surgeon.
A useful technique for bimanual cortical aspiration is what we call the POPS technique. POPS is an acronym for position, occlusion, posterior detachment, and swiping. The first step is to position the aspiration port so that its tip is under the anterior capsular fibers, pointed in the direction of the capsular fornix. Care is taken to maintain a safe distance from the capsular edge and posterior capsule. The anterior cortical fibers are then occluded with a gradual buildup of vacuum.
Once the port is completely occluded, the fibers are pulled posteriorly to detach them from the anterior capsule. After this, circumferential arc-like swiping movements are performed to further detach these fibers from the capsular fornix. Then the vacuum is escalated, the aspiration port is brought to the center, and the fibers are aspirated completely (see Watch It Now).
We prefer to use linear vacuum and flow rate for cortex aspiration. The preset parameters for cortical aspiration that we use are as follows:
- Vacuum, 300 to 400 mm Hg;
- Aspiration flow rate, 20 to 25 cc/min; and
- IOP, 40 to 50 mm Hg (bottle height 80–90 cm).
The conventional technique of centripetal pulling of cortex will detach the anterior subcapsular fibers; however, the pulling will cause the fibers to break off from their attachment to the equatorial cells, resulting in residual LECs remaining in the equatorial regions. In the POPS technique, the aspiration port is positioned under the anterior capsular fibers with its direction toward the fornix. With gentle buildup of vacuum, the anterior cortical fibers are occluded and subsequently displaced posteriorly. This detaches the fibers from the anterior capsule. Then with circumferential swiping movements they are further detached from the capsular fornix. Thus, this maneuver removes the lens fibers and epithelial cells in toto from both the anterior and posterior capsule. It has been demonstrated that these circumferential movements exert no traction on the zonules, unlike radial pulling forces.9 Once the fibers are detached, the port is brought to the center and the cortical material is aspirated completely.
The POPS technique can be performed in the setting of manual phacoemulsification, femtosecond laser-assisted cataract surgery, or small-incision cataract surgery with either bimanual or coaxial I/A techniques. It also has extended applications, especially in eyes with corticocapsular adhesions or zonular weakness.
The POPS technique can be particularly helpful for cortex removal in femtosecond laser-assisted cataract surgery. Because the firing of the laser leaves behind a sharply cut edge of cortical sheet without free ends of cortical fibers, cortex removal can be difficult in these cases. Adhering to the POPS technique helps the surgeon to occlude the cortical sheet effectively by positioning the aspiration port beneath the edge of the sheet rather than holding free fibers and pulling them radially.
CORTICOCAPSULAR ADHESIONS
One of the biggest snags in effective cortical removal is corticocapsular adhesions. These are defined as dense adhesions between the capsular bag and the lens material (Figure 1). Corticocapsular adhesions can result in zonular weakness or dehiscence, difficulty in nuclear rotation, and difficulty in achieving complete cortex removal.
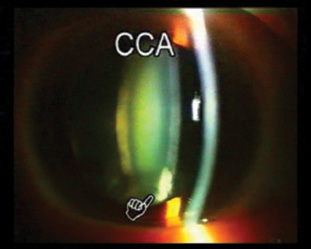
Figure 1. Corticocapsular adhesions are dense adhesions between the capsular bag and the lens material.
It is crucial to identify corticocapsular adhesions preoperatively so that the surgeon can deal with them effectively and avoid intraoperative complications. They are best detected on slit-lamp examination with oblique illumination and the slit beam angled at 45°.
Multiquadrant hydrodissection is effective in eyes with these adhesions. In this technique, multiple injections of small amounts of fluid are performed in different quadrants. Specially designed bent cannulas (Pricon) can be used for this maneuver (Figure 2). Multiquadrant cortical-cleaving hydrodissection should be performed in all eyes with corticocapsular adhesions, as well as in the event that the nucleus does not rotate with ease. Forceful nucleus rotation in the presence of corticocapsular adhesions can lead to zonular weakness or even disinsertion.
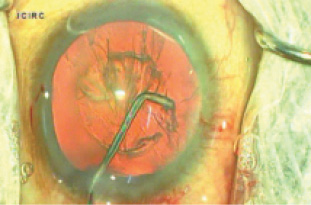
Figure 2. Multiquadrant cortical cleaving hydrodissection can be performed with a specially designed bent cannula.
It is important to remember that hydrodissection can be performed at any step during cataract surgery, whenever the surgeon encounters difficulty with nucleus rotation. Whenever the nucleus does not rotate, whether during sculpting, nuclear division, or nuclear fragment removal, the surgeon should stop, withdraw the phaco tip, and repeat hydrodissection. Proceeding further despite difficulty with nucleus rotation can lead to zonular loss.
CONCLUSION
It is important to have a technique for cortex aspiration that is safe, effective, and predictable in the surgeon’s hands. We recommend performing bimanual I/A, which provides superior surgical control during subincisional cortex removal and may be useful in complicated situations. Irrespective of whether the surgeon prefers bimanual or coaxial I/A, the POPS technique can help to achieve complete cleanup of cortex and LECs, ensuring a clear visual axis.
1. Nanavaty MA, Spalton DJ, Boyce J, Vasavada AR. Islands of lens epithelial cells on the posterior capsule in pseudophakic eyes. J Cataract Refract Surg. 2010;36(7):1135-1141.
2. Paik JY, Shiloach M, Macsai-Kaplan MS. The effect of posterior capsule polishing on posterior capsule opacification. Invest Ophthalmol Vis Sci. 2012;53(14):6668.
3. Blomquist PH, Pluenneke AC. Decrease in complications during cataract surgery with the use of a silicone-tipped irrigation/aspiration instrument. J Cataract Refract Surg. 2005;31:1194-1197.
4. Brauweiler P. Bimanual irrigation/aspiration. J Cataract Refract Surg. 1996;22:1013-1016.
5. Dewey SH. Cortical removal simplified by J-cannula irrigation. J Cataract Refract Surg. 2002;28:11-14.
6. Sakamoto T, Shiraki K, Inoue K, et al. A simple, safe bimanual technique for subincisional cortex aspiration. Ophthalmic Surg Lasers. 2002;33:337-339.
7. Vasavada AR, Dholakia SA, Raj SM, Singh R. Effect of hydrodissection alone and hydrodissection combined with rotation on lens epithelial cells; surgical approach for the prevention of posterior capsule opacification. J Cataract Refract Surg. 2006;32(1):145-150.
8. Peng Q, Apple DJ, Visessook N, et al. Surgical prevention of posterior capsule opacification. Part 2: enhancement of cortical cleanup by focusing on hydrodissection. J Cataract Refract Surg. 2000;26:188-197.
9. Nakano CT, Motta AF, Hida WT. Hurricane cortical aspiration technique: one-step continuous circular aspiration maneuver. J Cataract Refract Surg. 2014;40(4):514-516.
