



When we use toric lenses to treat astigmatism during cataract surgery, accurate placement of the IOL on the steep meridian is critical for good outcomes. When we look at outcomes, even though toric IOLs are highly effective, there is still quite a bit of residual astigmatism in patients who have received toric IOLs (Figure). Preoperative corneal marking is, therefore, of the utmost importance in preventing IOL misalignment. If we are 10° off our target, for example, the patient already loses one-third of the astigmatism correction that was intended.1
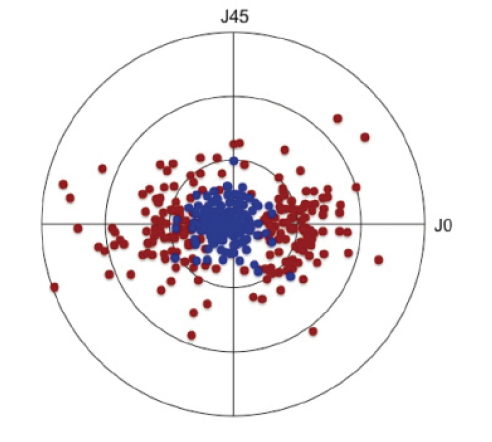
Figure. Corneal astigmatism before toric IOL implantation (red) and residual refractive astigmatism (blue) after toric IOL implantation. Each ring represents 1.00 D of astigmatism (n = 240 eyes).
We have little leeway, therefore, when it comes to positioning the IOL on the steep corneal meridian. Inaccurate placement of the IOL can occur as a result of inaccurate preoperative marking of the horizontal meridian, inaccurate preoperative prediction of the correct axis for IOL alignment, and/or inaccurate surgical implantation.2 This article reviews five fundamentals for nailing the axis alignment in toric IOL surgery.
1. Identify the Steep Meridian
Identifying the steep meridian is no easy task, especially in patients with low to medium amounts of astigmatism, because the nearly spherical shape of the cornea in these patients causes lower reproducibility of measurement methods. Additionally, measurement with different machines can lead to varying results, as can measuring only the anterior surface and disregarding the posterior corneal astigmatism.
Most of the error in managing astigmatism with toric IOLs occurs as a result of preoperative measurement inconsistency or imprecision. There is great variability of results among measurement devices, introducing increased risk for residual astigmatism. We need to get better at preoperative assessment concerning the actual astigmatism.
2. Toric IOL Calculation
Proper toric IOL power calculation that takes the posterior surface into account is the next crucial step in managing patients with astigmatism. Regardless of whether you have measured the posterior surface with swept-source OCT or some other method, the posterior surface should be taken into account when calculating the IOL power.
Keep in mind that the posterior surface typically has a lot of with-the-rule astigmatism. At least two different measurement devices should be used so that you have an idea of the irregularity of the cornea and so that you have a second measurement as a backup. If there is a big discrepancy between the two measurements, it may be necessary to perform them again at a later time. If the cause of the poor measurement is dry eye, lubricating drops should be used.
Swept-source OCT imaging devices such as the Casia (Tomey) or the IOLMaster 700 (Carl Zeiss Meditec) can improve accuracy in measuring low astigmatism. The scan speed in swept-source instruments is twice that in spectral-domain OCT devices, enabling the user to capture images of structures that were previously unattainable.
3. Marking Before Surgery
The processes of marking and positioning a toric IOL on axis during surgery can create a compounding of errors, leading to malpositioning of the IOL. Marking the horizontal meridian before surgery is a necessity because of cyclotorsion, and there are several methods that can be used for this. At the slit lamp, a needle can be used to make two small scratches at the periphery of the cornea, where the slit beam goes exactly through the pupil center, and then a color pen can be used to mark those scratches to ensure their visibility at the time of surgery. Other tools for marking the cornea preoperatively include pendulum markers, bubble markers, and tonometer markers.
Needle marking at the slit lamp works relatively well; be cautious, however. Slight inaccuracies during marking can create 5° to 10° of error right there and then. Whatever manual marking technique you use, it is important that you make sure you are achieving reproducible results with it.
4. Markerless Approach
Automated systems, such as the Callisto eye (Carl Zeiss Meditec), Verion Image Guided System (Alcon), IntelliAxis-L system upgrade to the Lensar Laser System (Lensar), and the ORA with VerifEye+ (Alcon) can enhance workflow and precision in surgical preparation. Photos taken of the eye before surgery can be integrated with your biometry machine, which also measures the keratometry and the astigmatic axis with the patient in the sitting position. The automated system can then match the images taken during biometry with the live image coming through the oculars of the microscope during surgery.
The images taken prior to surgery show landmarks on the eye that are matched to the live intraoperative image, which can give you a precision of within 1° or less.3 Typically, these systems also have an automated tracking system so that, when the eye is rotated during the surgery, the horizontal and the target meridians are adjusted in real time. This provides the surgeon with a live image with the steep meridian superimposed in the microscope’s eyepiece, optimizing the surgeon’s ability to place the IOL in the targeted position.
5. Position the IOL
Positioning the toric IOL on the steep meridian is a three-step procedure that involves gross alignment, removal of the OVD, and final alignment. For gross alignment, the IOL is rotated clockwise to approximately 5° to 10° short of the desired position. The IOL is then stabilized during OVD removal; care should be taken to prevent the IOL from rotating past the intended axis while removing the OVD. After the OVD has been removed from behind the IOL, final alignment can be done. The IOL is carefully rotated clockwise, precisely onto the intended axis of alignment, with the infusion running.
CONCLUSION
Paying attention to these five fundamentals will help to ensure successful toric IOL implantation with good postoperative results for your patients with astigmatism.
1. Hill W, Potvin R. Monte Carlo simulation of expected outcomes with the AcrySof toric intraocular lens. BMC Ophthalmol. 2008;8:22.
2. Popp N, Hirnschall N, Maedel S, Findl O. Evaluation of 4 corneal astigmatic marking methods. J Cataract Refract Surg. 2012;38(12):2094-2099.
3. Varsits RM, Hirnschall N, Döller B, Findl O. Evaluation of an intraoperative toric intraocular lens alignment system using an image-guided system. J Cataract Refract Surg. 2019;45(9):1234-1238.



