

No existing IOL provides perfect visual acuity at all distances and under all levels of illumination. Aspheric monofocal lenses achieve the best retinal image contrast but the narrowest depth of focus. Presbyopia-correcting lenses increase depth of focus and focal range, but they offer poorer retinal image contrast and will induce dysphotopsias. How great the tradeoff is generally correlates to how great a range of focus an IOL is designed to provide. For example, a low-add multifocal or extended depth of focus (EDOF) lens typically compromises retinal image quality less than a high-add multifocal lens. No currently available lens provides the retinal image quality of an aspheric monofocal lens across the full range of distances from infinity to near.
The retinal image of each of a person’s eyes is symmetrical but not identical. Small interocular differences in retinal images are fused in the visual cortex to enhance binocular visual perception. Current dogma holds that the same IOL should be implanted in each of a patient’s eyes, but it is important to recognize that doing this does not produce identical retinal images in the two eyes. Small but inevitable interocular differences in defocus, astigmatism, higher-order aberrations, and biometric parameters can translate into significant differences in the retinal images produced.
This is where binocular customization comes into play. The goal of binocular customization is to produce retinal images in each eye within a fusion-compatible range so that the patient can achieve the full range of functional vision while minimizing the tradeoff in quality of vision. This can be accomplished by combining almost any lens designs or by using the same lens design with a defocus target modulation between the eyes, such as is used in monovision. Investigators have reported excellent results from combining refractive and diffractive multifocal IOLs,1 monofocal and multifocal IOLs,2 and EDOF and multifocal IOLs.3
Preoperative counseling is crucial for successful bilateral customization. Patients must be primed to expect small differences in the visual acuity of their eyes and understand that these differences are purposeful to improve binocular performance.
STRATEGY IN PRACTICE
The overall concept in bilateral customization of IOL selection is to achieve the widest range of vision binocularly while minimizing how much quality of vision is compromised. I base my binocular customization strategy on panfocal visual acuity testing. This functional vision measure can define lens performance at the 95th percentile, and it also provides a detailed framework that helps me to identify gaps in vision and potential issues with quality of vision.
In general, I start with the patient’s worse-seeing eye and a refractive target of emmetropia. I select an EDOF IOL (Tecnis Symfony, Johnson & Johnson Vision), a trifocal IOL such as the FineVision trifocal (PhysIOL) or AcrySof IQ PanOptix Trifocal (Alcon), or a hybrid EDOF multifocal lens (Tecnis Synergy, Johnson & Johnson Vision) based on which of these will provide the equivalent of a +2.50 D add for that particular eye.
I ask patients to function without spectacles for approximately 1 week after surgery on their first eye before being assessed for surgery on their second eye. The customization process for the second eye depends on their feedback and the results of panfocal visual acuity testing. I find that patients usually follow one of four routes (see Four Routes to Satisfaction ).
Four Routes to Satisfaction
Typical situations after surgery on a patient’s first eye.
No. 1: The patient is happy with his or her range of vision and experiences no problems with dysphotopsias. I will use the same lens and refractive target for the second eye as I did for the first eye.
No. 2: The patient is happy with his or her distance visual acuity and experiences no problems with dysphotopsias but desires better near visual acuity. I will implant an IOL that emphasizes near visual acuity in the second eye. Options include the FineVision trifocal (PhysIOL), AcrySof IQ PanOptix Trifocal (Alcon), or Tecnis Synergy (Johnson & Johnson Vision).
No. 3: The patient is happy with his or her near visual acuity but desires better distance visual acuity. I will implant either a Tecnis Symfony (Johnson & Johnson Vision) or a Tecnis Eyhance (Johnson & Johnson Vision), an enhanced monofocal IOL, in the second eye.
No. 4: The patient is happy with his or her near visual acuity but is concerned about halos and driving at night. I will implant either an aspheric monofocal lens or a Tecnis Eyhance in the second eye to encourage neural adaptation by eliminating halos and glare from one eye.
Binocular customization doesn’t require the use of two different IOLs in every case. Most of my patients receive the same lens in both eyes because they are happy with the results of surgery on their first eye. The optimization process enables me to consider which lens will achieve the best binocular visual outcome.
In 2018, I most often implanted the Tecnis Symfony bilaterally using a nanovision approach (ie, correction of the dominant eye to emmetropia and the nondominant eye to -0.50 D. All patients achieved distance and intermediate visual acuity of 6/9 or better, 96% achieved near visual acuity of 6/9 or better in photopic conditions, and 74% achieved near visual acuity of 6/9 or better in mesopic conditions (Figure 1). More than 95% of these patients could carry out all intermediate and near vision tasks in photopic and mesopic conditions except for reading a newspaper under mesopic conditions (88% could perform this task) and reading a telephone book under mesopic conditions (65% could perform this task; Figure 2).
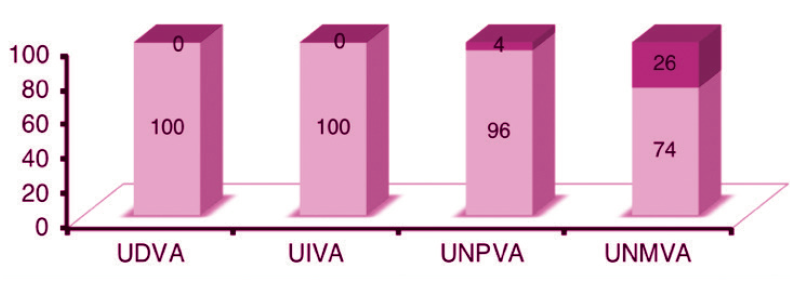
Figure 1. Personal data on binocular implantation of a Tecnis Symfony lens using a nanovision approach and panfocal vision testing.
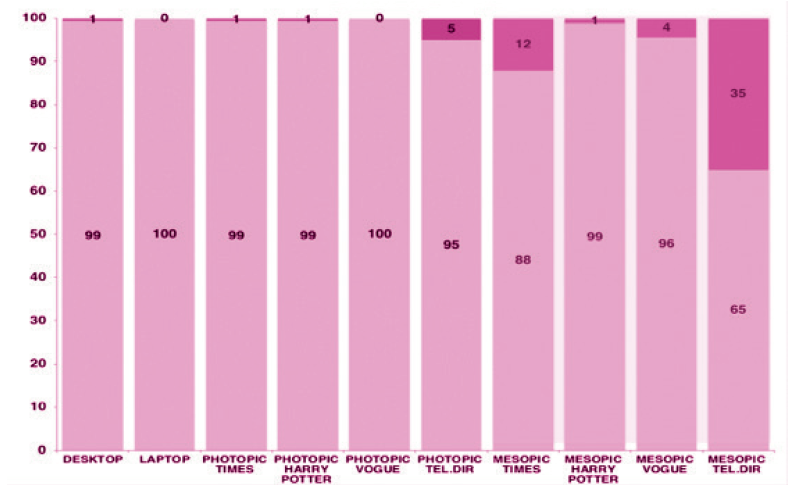
Figure 2. Personal data on objective task assessment after the implantation of a Tecnis Symfony IOL in each eye using a nanovision approach.
CONCLUSION
Binocular customization is critical in achieving excellent functional vision outcomes. As new IOLs with better functionality enter the market, the customization process will evolve to include these options.
1. Goes FJ. Visual results following implantation of a refractive multifocal IOL in one eye and a diffractive multifocal IOL in the contralateral eye. J Refract Surg. 2008;24(3):300-305.
2. Iida Y, Shimizu K, Ito M. Pseudophakic monovision using monofocal and multifocal intraocular lenses: hybrid monovision. J Cataract Refract Surg. 2011;37(11):2001-2005.
3. Black S. A clinical assessment of visual performance of combining the TECNIS Symfony Extended Range of Vision IOL (ZXR00) with the +3.25 D TECNIS Multifocal 1-piece IOL (ZLB00) in subjects undergoing bilateral cataract extraction. Clin Ophthalmol. 2018; 12:2129-2136.
