
CASE PRESENTATION
A 72-year-old man presented with a history of decreasing visual acuity and difficulty reading street signs. On examination, his BCVA was 20/60 OD with a manifest refraction of +1.00 -2.00 x 110º and 20/100 OS with a manifest refraction of -1.00 D sphere. Iris transillumination defects were evident in both eyes. A 2+ brunescent nuclear sclerotic cataract was present in the right eye, and a 3+ nuclear sclerotic cataract with a 3+ posterior subcapsular cataract was present in the left eye. There was pseudoexfoliative material on the anterior capsule in the right eye, and the pupil of the left eye dilated poorly. The remainder of the examination was unremarkable, as was OCT imaging of the maculas and optic nerves. After a discussion of the risks and benefits of cataract surgery, the patient elected to proceed with laser cataract surgery on the left eye and implantation of a toric IOL to correct approximately 1.00 D of corneal astigmatism.
On the day of surgery, the pupil remained small despite the instillation of additional dilating drops. A laser capsulotomy with the LenSx Laser (Alcon) was successful, with the normal size of 5.0 mm decreased to 4.6 mm because of the poor pupillary dilation. Intraoperatively, severe instability of the lens was evident during removal of the free-floating capsulotomy and during gentle hydrodissection of the nucleus and cortex with balanced saline solution. The patient was asked about a history of trauma to the eye. He stated that he had forgotten to mention at the original evaluation that he had sustained blunt trauma to the left eye several months earlier and that it had resulted in loss of vision and “seeing stars” for a few minutes.
The patient desires distance correction with a toric IOL. How would you proceed?
—Case prepared by Cathleen M. McCabe, MD

ASHVIN AGARWAL, MS
I generally find retaining the capsular bag to be in the best interest of the patient. I would select a three-piece IOL for this patient but would be prepared to perform an anterior vitrectomy if necessary. After entering the eye, I would place one or two capsular hooks with or without a capsular tension ring (CTR) to promote safe removal of the nucleus and cortex. Next, I would analyze the quality of the capsular bag (eg, strength of the zonules, texture, sheen) and assess the clock hours of instability. If the amount of subluxation is less than 5 clock hours, then I would insert a CTR (Figure 1) at the capsular equator and place a Jacob Paperclip Capsule Stabilizer (Morcher) at the rim of the capsulorhexis. The double-looped end of the hook is slid like a paperclip over the anterior capsular margin (Figure 2). The haptic-tipped end is externalized through a partial-thickness scleral flap and sclerotomy and then tucked into a Scharioth tunnel parallel to the limbus (Figure 3), thus stabilizing the bag in those clock hours of weakness. A toric IOL can then be implanted and positioned in the bag, and the capsular hooks can be removed, permanently leaving behind the paperclip hook. I find that this technique works best when I do not need to use sutures to stabilize the capsular bag-IOL complex. If the amount of subluxation is 5 clock hours or more, then I consider other options.
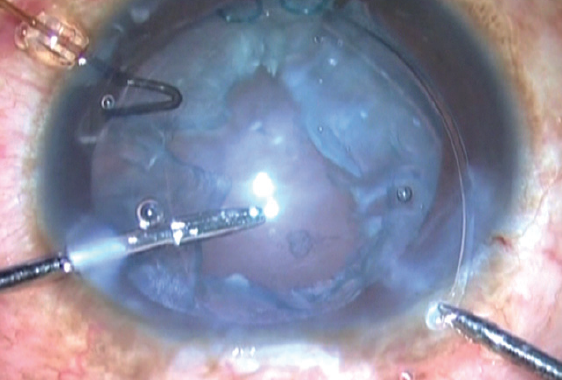
Figure 1. Dr. Agarwal uses a CTR in eyes with less than 5 clock hours of zonular instability.
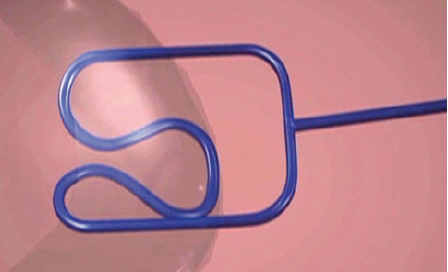
Figure 2. The double-looped end of the paperclip hook slides over the anterior capsular margin.
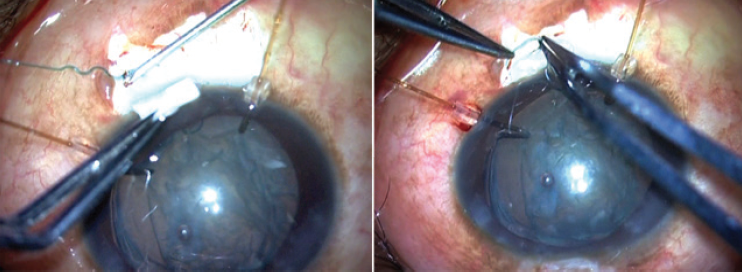
Figure 3. The haptic-tipped end of the paperclip hook is externalized through a partial-thickness scleral flap and sclerotomy and then tucked into a Scharioth tunnel.
All figures courtesy of Ashvin Agarwal, MS

MICHAEL E. SNYDER, MD
Although hydrodissection has been completed, instilling a highly dispersive OVD into the equator of the capsular bag will help stent open the bag a bit and reduce the risk of inadvertent aspiration of the equatorial bag during phacoemulsification. Placing capsular hooks in the four oblique quadrants via paracenteses will support the equatorial bag, after which nuclear emulsification can be undertaken. I would be cautious not to overtighten the hooks so as to avoid placing undue stress on the capsulotomy because a laser capsulotomy does not have as much tensile strength as a continuous curvilinear capsulorhexis.
After performing nuclear removal, I would aspirate the cortex and strip the strands tangentially in the most zonule-friendly manner possible. A fixable capsular element such as a Malyugin/Cionni CTR or Ahmed Segment (both from Morcher) or an AssiAnchor (Hanita Lenses) could then be placed into the capsular bag and the fixation element secured to the eye wall with a nonabsorbable suture. Given the diffuse zonulopathy, two or more fixation elements may be required. The capsular hooks can be disengaged and removed and the IOL placed in the bag, after which the globe is pressurized and the suture tension adjusted at each location to center the lens implant. The fixation sutures should be fully locked and the knots rotated internally. I would then aspirate the OVD from behind the IOL and center the IOL to (what I hope is) the premarked steep axis. The OVD could then be removed from the anterior chamber. I would instill intraocular carbachol to blunt an IOP increase on postoperative day 1.

WHAT I DID: CATHLEEN M. MCCABE, MD
I increased capsular support and pupillary dilation by using an XpandNT Iris Speculum (Diamatrix) to capture both the pupillary and capsular margins. This thin nitinol ring opens to 6.7 mm and can gently cradle the pupillary margin alone or in combination with the anterior capsular rim in cases of zonular instability.
Once the capsule was supported, phacoemulsification and cortical removal proceeded in a normal fashion. A preloaded Morcher EyeJet Type 15A CTR (Morcher) was placed in the capsular bag, followed by an AcrySof IQ Toric IOL (Alcon) that was rotated to the correct axis. A cut segment of a 5-0 polypropylene suture was melted with low-temperature cautery into a flange at one end and threaded through the eyelet of an Ahmed Segment. The Ahmed Segment was placed inferiorly into the capsular bag. The iris speculum was disengaged from the pupillary and capsular margins inferiorly, nasally, and temporally, leaving the superior margin engaged to support the capsule.
The sulcus was inflated inferiorly with an OVD. A 27-gauge needle was placed through the conjunctiva and sclera 2 mm posterior to the limbus inferiorly and into the sulcus in front of the capsular bag. The free end of the 5-0 polypropylene suture was inserted into the anterior chamber and threaded into the lumen of a 27-gauge needle, which was withdrawn from the sclera and conjunctiva. The polypropylene suture was grasped at the level of the conjunctiva, trimmed, and melted into a flange with low-temperature cautery. A similar technique was used to fixate a second Ahmed Segment to the sulcus with a 5-0 polypropylene suture located 180º superiorly to the inferior segment, thus securely fixating the IOL-capsular bag complex to the sclera in the sulcus.
It is important to carefully titrate tension on the suture through the eyelet of the Ahmed Segment. The appropriate tension will support the anterior capsule without significantly distorting the contour of the capsular rim.
The flanges were then pushed through the conjunctiva to lie flush with the sclera. I confirmed this by smoothly running a cannula over the conjunctiva in the area of each flange. I instilled carbachol in the anterior chamber at the end of surgery. On postoperative day 1, IOP was 16 mm Hg, and uncorrected distance visual acuity was 20/30+2.
Canabrava and colleagues described the use of a 5-0 polypropylene suture to fixate Ahmed Segments to the capsular bag.1 This technique provides very stable sulcus fixation without the need for a peritomy or sclerotomy. In this case, the laser capsulotomy had a diameter of 4.6 mm, which meant that a significant amount of stress was exerted on the capsular margin to accommodate the size of the pupil expander. It is worth noting that the capsule was able to withstand this stress without tearing.
1. Canabrava S, Bernardino L, Batisteli T, Lopes G, Diniz-Filho A. Double-flanged-haptic and capsular tension ring or segment for sutureless fixation in zonular instability. Int Ophthalmol. 2018;38(6):2653-2662.
