


1. The gender gap in ophthalmology is shrinking. What, in your opinion, can this be attributed to?
Lisa Brothers Arbisser, MD:
It’s attributed to both an increase in the number of women in medical school and the prestige and attraction of the ophthalmology specialty. The mix of medicine and surgery, the ability to see all ages and genders of patients (without the need to disrobe), and the low emergency nature of the field makes it particularly attractive and well-suited to women, who often seek a work-life balance that much of the practice of medicine does not afford. The delicate and exacting nature of the surgery is also appealing.
Allon Barsam, MD, MA, FRCOphth:
There are a variety of factors. There is generally more equality regarding gender from medical school, and that carries through to the workplace. People discriminate much less now based on gender than they used to.
There’s also more sharing of responsibilities between men and women when it comes to things like family and child care. It doesn’t always fall only on the woman to do everything or even the majority of what’s required for raising children.
It’s become easier and more acceptable to work flexibly, even in medicine. And there is more role- modeling. When people of one gender don’t have someone in their gender to look up to who does what they want to do, that makes it harder for them to envision themselves in that job or that role. With more women in ophthalmology, there are more women role models to look up to.
I think there is more of a gender gap in ophthalmology in the United States than there ever has been in the United Kingdom. However, in the UK private sector, where all refractive surgery is performed, it’s a bit more uneven. I think one reason for this may be that often the time demands for refractive private practice work are greater, and that may be an issue because historically men have been more prepared to work longer hours with women being more responsible for child care.
Björn Johansson, MD, PhD, FEBO:
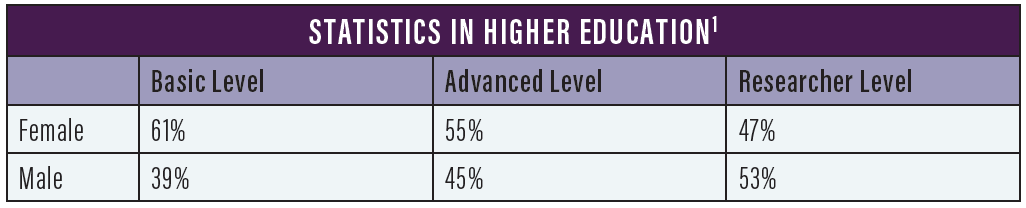
At universities, the situation for men and women has changed quite a lot in the past 50 years. There are more female than male students right now,1 which suggests that we will eventually close the gender gap in higher education (see Statistics in Higher Education).
Work-life balance has also changed. As a medical resident now in Sweden, it’s quite common for both men and women to have a part-time schedule that allows individuals with small children to take 25% of time off from the job. You can negotiate to take 1 day a week or 2 afternoons off. Many of my colleagues who are young parents use that option. In ophthalmology, a high-volume specialty, you can see many patients in part of the day.
In my early years, that was not so. You were expected to use your time at the clinic to learn, to see as many patients as possible, to perform surgery, and to study. And now, that’s still important, but it’s also recognized that it is important to watch your children grow up, not just to say goodnight to them or eat dinner and breakfast with them.
I see both genders taking advantage of this arrangement. I notice that situations are more similar for both genders than they were 50 years ago, and in the end, I believe this will lead to more equal possibilities for both males and females to build their careers.
A. John Kanellopoulos, MD:
Regardless of gender, clinicians achieve excellence through passionate work and tireless care for their patients. Considering the obviously unequal burdens that women have as mothers, especially with young children, ophthalmology can be a specialty more attractive to women who decide to have a family parallel to their professional careers. This is because most of our clinical work can be scheduled. As far as our everyday routine in practice, there is essentially no difference between men and women in our function and working environment in general.
Aylin Kılıç, MD:
The gender gap in ophthalmology is not shrinking in all countries. People are more aware of the issue in some situations and societies, but in some countries it is still a real issue. Some industries have become sensitive to the gender gap. But depending on the cultural or political situation in many areas, the preference is still more for men to achieve higher positions than for women.
Marguerite B. McDonald, MD, FACS:
My view on this is very pragmatic: Now, with more women in ophthalmology than ever before, it is hard to ignore a so-called minority group that is this large. (Read more of Dr. McDonald’s thoughts on challenges faced by women in her accompanying sidebar.)
The Challenges of Yesterday
Lessons learned in a satisfying career in ophthalmology.
By Marguerite B. McDonald, MD, FACS
I was attracted to a life in medicine because my dad was an orthopedic surgeon and the director of the local ER; he clearly took great joy in his work. Dad came home every night with incredible stories, mostly with happy outcomes. Some days, though, he would go straight to the living room, sit in his favorite lounger, and stare silently at his clenched hands for hours. These were the days when mom whispered, “Dad had to tell another set of parents that their son died in a motorcycle accident.”
Ophthalmology interested me because I had significant bilateral vision issues as a child. I was treated successfully, and I saw clearly for the first time when I was 5. Eventually, I decided that I wanted to do for others what had been done for me.
I hesitate to tell stories from my early days in medicine because young women won’t face most of the challenges that I faced—though they will still face some of them. Also, telling these shocking stories makes me seem older than Methuselah, even though they took place not so long ago.
THE PLAYING FIELD
The overall picture is now better for women in medicine, but the playing field is still not flat. I recently read an article about the gender pay gap among general surgeons.1 It was a well-done study with equal numbers of male and female surgeons enrolled. The surgeons had all done similar residency and fellowship training in prestigious programs, they worked the same number of hours each week in the office and in the OR, and they performed the same number of cases. Yet the male surgeons earned significantly more money than the female surgeons. The investigators discovered that most of the cases with high reimbursement potential went to the male surgeons and most of the low-reimbursement cases went to the female surgeons. In their conclusion, the investigators stated that the next goal of their research is to discover why this occurs: Is it that male physicians like to refer the high-reimbursement cases to other male physicians, or do the high-reimbursement cases get referred to the male doctors at the point when the calls come in to the switchboard or front desk staff? I am eager to read their next article.
I do not regret my choice of career in medicine or in my choice of ophthalmology in particular. It has been an honor, a challenge, a privilege, and a joy. Our field changes so quickly—for the better—that one feels the need to catch up after even a 1-week vacation! It is crucial to constantly learn new things, whether it is about drug therapies, surgical techniques, or in-office procedures.
Our specialty requires knowledge, courage, self-confidence, and dedication. We make intraoperative maneuvers that require micron and submicron accuracy, so our hand-eye coordination must be impeccable. Most of us take this responsibility very seriously; we go to bed early the night before surgery and forgo the glass of wine with dinner.
Women have these characteristics, just as men do, but we can sometimes be a bit low on self-confidence and courage. As an ophthalmologist friend of mine said, “If we women have a surgical case that doesn’t go quite the way we planned, we instantly doubt whether we should even be surgeons. My male colleagues are similarly distressed in this situation but manage to shrug it off as a bad day in the OR.”
Courage is a critical ingredient in the secret sauce of success. To quote Franklin Delano Roosevelt, “Courage is not the absence of fear, but rather the assessment that something else is more important than fear.”
1. Dossa F, Simpson AN, Sutradhar R, et al. Sex-based disparities in the hourly earnings of surgeons in the fee-for-service system in Ontario, Canada. JAMA Surg. 2019;154(12):1134-1142.
Marie-José Tassignon, MD, PhD, FEBO, FEBOS-CR:
It is very difficult to say that there is a gender gap. In my career, I must state emphatically that I haven’t seen so much difference between men and women. But the many people who defended women in the past deserve the most credit for the current situation.
Another factor is that boys and girls are now educated in the same schools.2 I was well beyond school age when schools became coeducational in the 1980s or even later. I don’t believe that there is a gender difference in intelligence. I think women and men have the same capacity, but they have been educated differently for centuries.
Denise M. Visco, MD, MBA:
The shrinking gender gap is attributable to the gains women have made in the dimensions of educational attainment, occupational segregation, and work experience.3 I don’t think that ophthalmology is unique or different from the rest of Main Street; if anything, we are lagging.
2. Even though the number of women in the field of ophthalmology is growing, the percentage of women department chairs, full professors, researchers, speakers, and practice owners is still relatively low. What can female ophthalmologists do to improve this? How about male ophthalmologists?
Dr. Arbisser:
As far as looking at achievements in ophthalmology, I think that has been more difficult for women. Whether that’s history, a glass ceiling that needs to be broken, or the undeniable commitment of time to the surgical aspect of our specialty, something has held us back a little bit. It’s all circular in that the more volume you do, the better surgeon you are, the more you’re important to industry, the more you teach, the more you learn, and the more patients will come to you. That can be challenging for anyone who’s trying to lead a balanced life, which tends to be more women than men in my experience.
I was able to excel at that challenge at a time when there were very few women in our specialty. This is partly because of the great partnership I have with my husband of nearly 50 years, who saw my talent and helped to promote me. He convinced me I didn’t need to see routine patients all the time or conduct every single postoperative visit, which allowed me to make room in my schedule for more surgery. He was able to put aside hubris, and I was able to step up to the task. Where men still dominate, they have to be sufficiently secure and prescient to step aside and make room for women when appropriate. Women didn’t get the vote in this country on their own! Despite the suffrage movement, success required men voting for it! Today, there are more women who understand how to prioritize their goals, and they are striving to achieve those goals for themselves. But our progress in general still depends on the men—often in charge—making room for us and recognizing that this is often to their own advantage.
Dr. Kılıç:
Whatever we do to improve the number of females in leadership positions, it is difficult or sometimes impossible to succeed without political support in a given environment. Female ophthalmologists with established careers must support young female ophthalmologists by giving them educational opportunities and career assistance. If we feel that a candidate deserves our support for career development, we should provide that support equally, regardless of gender.
Dr. McDonald:
There are three factors that have helped women in ophthalmology to advance in their careers and positions:
No. 1: Demonstrating an overarchingly superior job performance;
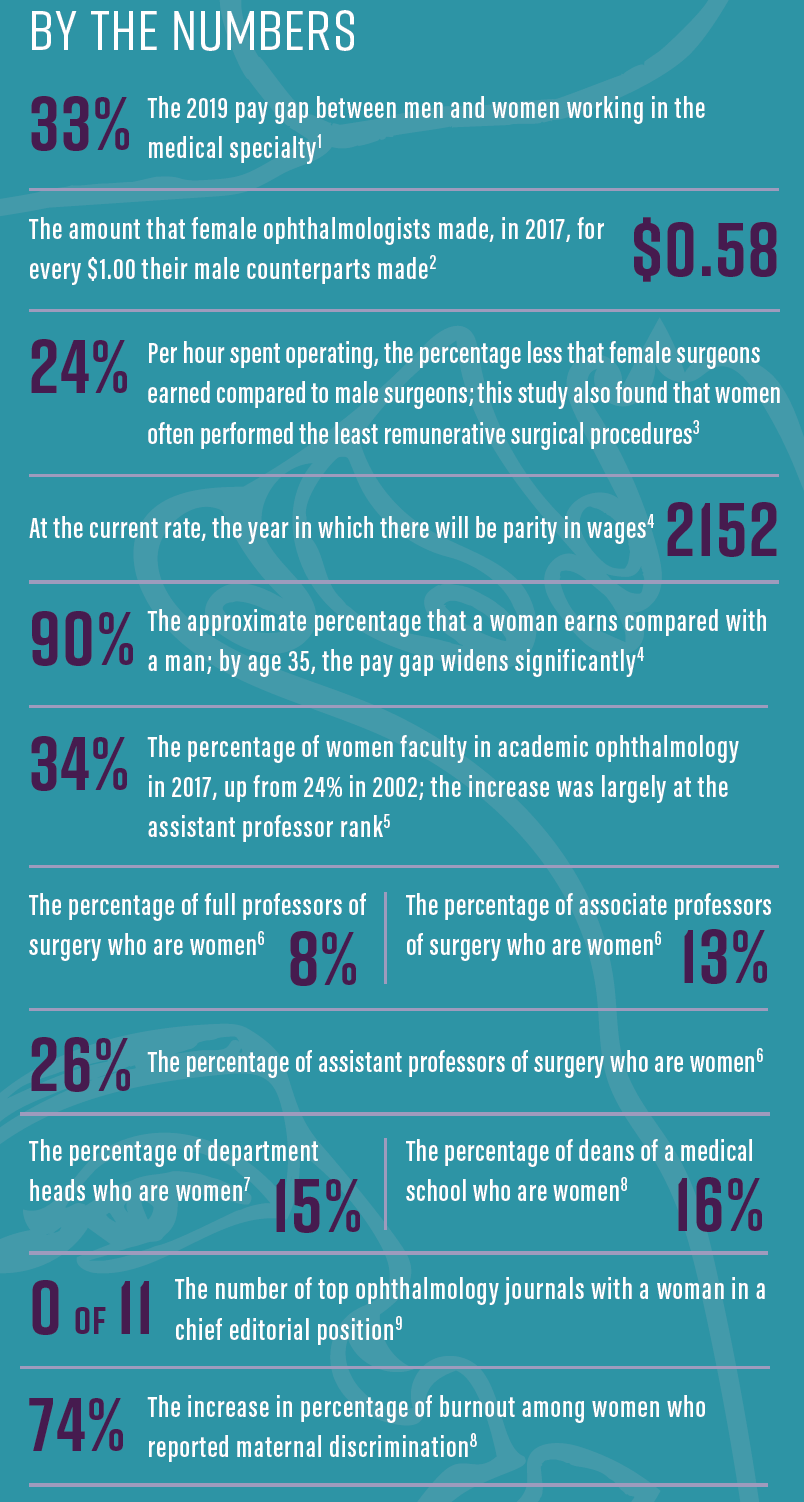
No. 2: Being fully aware of the presence of the gender gap, including the differences between men and women in social, political, and economic attainments (see By the Numbers), as knowing the facts can assist women in their requests for advancement; and
1. Ducharme J. The gender pay gap for doctors is getting worse. Here’s what women make compared to men. Time. April 10, 2019. https://time.com/5566602/doctor-pay-gap/. Accessed April 13, 2020.
2. Reddy AK, Bounds GW, Bakri SJ. Differences in clinical activity and Medicare payments for female vs male ophthalmologists. JAMA Ophthalmol. 2017;135(3):205-213.
3. Dossa F, Simpson AN, Sutradhar R, et al. Sex-based disparities in the hourly earnings of surgeons in the fee-for-service system in Ontario, Canada. JAMA Surg. 2019;154(12):1134-1142.
4. Gender Equity Toolkit. Association of Women Surgeons. https://www.womensurgeons.org/page/GenderEquity. Accessed April 13, 2020.
5. Tuli SS. Status of women in academic ophthalmology. J Acad Ophthalmol. 2019;11(2):e59-e64.
6. Why AWS is important. Association of Women Surgeons. https://www.womensurgeons.org/page/WhyAWSisImportant. Accessed April 13, 2020.
7. Year of reckoning for women in science. Lancet. 2018;391(10120):513.
8. ‘A banner year:’ Women leaders established in ophthalmology. Ocular Surgery News. September 29, 2017.
9. Gordon L. Building diversity in medicine and ophthalmology. Paper presented at: Women in Ophthalmology Annual Meeting. August 23, 2019; Coeur d’Alene, Idaho.
No. 3: Speaking up and letting our wishes be known, including vocalizing what boards you’d like to be on, what title you would like to have, and what talks you would like to give.
Magda Rau, MD:
In former Iron Curtain countries, ophthalmologists have traditionally been mostly women, but leadership positions such as chiefs of departments and university clinics were mostly held by men. It may have been prejudice that led to this, but the biological difference for producing children and likely desire for part-time positions are also factors.
Professor Tassignon:
I have been the director of educational programs in ophthalmology at Antwerp University Hospital since 1991. I have seen good male and female students who were excellent in their jobs, clinics, and surgery but who were not interested in educational leadership. During training, men with leadership capacities were often not interested in neuro-ophthalmology, low vision, or pediatric ophthalmology. They wanted to attend the surgical program but then claimed they were sick during educational topics they were not interested in. Men often started their own private practices, giving them the ability to be solely responsible for practice preferences. They most often chose cataract and refractive surgery, making them completely dependent on their patients’ expectations. Who is fooling whom?
I do agree, however, that excellent female candidates for leadership positions hesitate to apply for a position for a variety of reasons: young age, unpreparedness, or incomplete education. These arguments are understandable, but all leaders take some calculated risks. Nobody is fully experienced at age 38.
It is, of course, difficult for those who have the responsibility to make the right choices for a leader. Some people just want to have the title, and they do not necessarily have the capacity. Each individual must be evaluated externally and pass psychological tests to decide whether he or she is a good candidate for a leadership position. Women can be valuable leaders, and if they let their desires known, hopefully, in the future, we will continue to see more directors, department heads, and full professors who are women and deserve it.
Dr. Visco:
Women are on par with men in getting medical and legal degrees, yet, across the board, men are far more likely to receive the most prestigious and highest-paying leadership rolls.4
Ophthalmology is unfortunately no different. A recent study found that female residents performed fewer cataract operations and total procedures than male residents.5 Ironically, the men who took paternity leave performed a mean 27.5 more cataract surgeries than those who did not take any leave. One good note was that the female residents’ numbers were neither enhanced nor penalized for taking maternity leave.
As the Association of Women Surgeons has stated, for the female ophthalmologist, “battling workplace bias requires deliberate strategies, including learning to say no, getting comfortable talking about uncomfortable topics, and helping others behind you.”6
There are things we can do. When you see bias occurring, discreetly make the individual aware of the biased behavior. Actively manage how others view you by learning and practicing leadership skills. Nurture relationships with other female mentors and support other women in senior roles. Finally, understand your workplace policies on discrimination and your rights.
My advice to male colleagues is to do your best in considering how you make decisions and choices. Gender bias is cultural, and we all should be mindful of our language and behaviors. Intervene when a female colleague is spoken over or demeaned. Make a point of showing your male colleagues the value of female contributors and promote a culture of gender-neutral meritocracy.
3. What are some ways that women can hone their effective leadership skills in the hope of advancing in rank within their practice or academic institution?
Dr. Arbisser:
There are many types of leadership, and leadership in surgery and leadership in organized medicine require different skills and tasks. Does a woman have to be president of an organization in order to be a leader? Not necessarily. It could be that a woman is making sure that people are doing the highest-quality work, and that is being a leader, too.
It might take our redefining what leadership can be in order for us to capture more of those leadership roles on the way to achieving our highest goals. Speaking up and getting noticed for quality is fulfilling; unfairly unrequited achievement is a stain upon our profession—whether that manifests as gender, religious, or racial bias.
Dr. Kılıç:
Male ophthalmologists must support female ophthalmologists in academic work and surgical positions. Women may sometimes be afraid to take the first steps toward a career because it involves a risk. Effective leadership should always demonstrate that it can be beneficial not only to take a risk but also to make mistakes to keep improving and building your career. Young female ophthalmologists need to hear people say, “You can do it.”
Dr. McDonald:
The best piece of advice I have to offer is to go above and beyond what people expect. Volunteer to take on more responsibilities, give more lectures to the residents than required, and ask to join teams and boards.
Dr. Rau:
In addition to the leadership skills mentioned by the other panelists, my recommendation is to employ a systematic method of enthusiastic work. Find a field and methods you are interested in. When you achieve good results—ie, satisfied and happy patients—then this supports your further work. The easiest way is to find a niche. But, in the future, women will want to achieve even more than just a niche.
Professor Tassignon:
Go back to school to gain more insights about leadership. It is very important to learn the aspects of leadership. You will have credentials to show if you want to apply for something, and you will have shown that you have an interest in leadership. I recommend this to anyone who shares with me the desire to lead.
Dr. Visco:
Leadership skills can be learned, and lateral leadership—the ability to influence others without formal authority—is extremely important for anyone wishing to advance his or her rank within an organization. Harvard Business Review recommends honing four key skills: networking, constructive persuasion, consultation, and coalition building.7 Cultivate a broad web of relationships based on mutual respect and ideas, learn how to negotiate with a win-win strategy, take time to visit with stakeholders and show interest in their opinions, and, finally, earn advocates who will support and stand by you. Another key point is that leadership learning, like all learning, should be lifelong. I am looking forward to attending the Harvard Medical School Women’s Leadership Conference this fall.
4. Are there certain perceptions and behaviors present in ophthalmology that contribute to the gender gap? What can be done to change these?
Dr. Arbisser:
Ophthalmology has a history of having an old boys’ club mentality, and, unless you aggressively barge your way in, you can be overwhelmed by the unfairness of it all. I was never invited to the residents’ poker game with the chairman. As long as there’s still that mentality, the gender gap will continue to some degree. Unless you’re able to cope with that and be a little more aggressive and demanding in other ways, it’s hard to overcome.
When the mix involves having children, our partners have to pull their weight and break out of that old paradigm that raising children is women’s work. It’s a juggling act, and there is always at least one ball in the air we are praying to catch.
Dr. BARSAM:
Of course we are making generalizations, but I think certain personality types may act as barriers. This may not be as true in ophthalmology as in other surgical specialties, but certainly the type-A alpha male surgeon personality being somewhat egotistical or controlling is a bit more common. This could describe, for instance, a refractive surgeon or high-volume cataract surgery personality type. Maybe this would be considered old-fashioned now, but it’s still prevalent. It may be that women have been put off by that.
I’m aware that there aren’t enough women practicing surgery in the United Kingdom, but I see no reason why there should be a gender gap. We should all acknowledge that any practice can be complemented by having a more broad representation of different gender, generational backgrounds, and races.
Dr. Johansson:
Hidden mechanisms in society contribute to the gender gap. In the culture at large, the image of an expert in many higher occupations is of a man, perhaps 50 or 60 years of age, wearing a suit and tie.
Another example is in sports. Just recently, on the Swedish national radio news channel, I listened to an interview with a female football trainer who was saying something like, “Women have been playing football at an advanced level for a long time by now. Still, the normal image of a football trainer is a man. So a female football trainer immediately evokes the reaction that she is outside the normal range for a football trainer, and you have to deal with that when you start doing your job.” There are female experts and opinion leaders in every industry. They may have been a minority, but they have been there.
So I think this unconscious image, for many people, depicts how things are. In general, we consider ourselves to have equality between the sexes, but some social constructions that have been in place for many years can present barriers to women.
Dr. Kanellopoulos:
Generally speaking, of course, ophthalmology has, for a long time, been one of the optimal specialties in medicine to bridge the gender gap, with others probably including microbiology, radiology, and dentistry.
Medicine has opened its arms and has engaged great women in specialties that might be perceived by the public as ones that only males are expected to excel in. For instance, in comparing general surgery to ophthalmology, the public may have in the past perceived the former as a heavy surgical specialty, as opposed to the delicate nature of the eye and the surgical detail required in eye surgery. Many people, for many years, have more easily accepted the idea of being treated by a female ophthalmologist. On the other hand, until several decades ago, many of those same people might not have wanted to have cardiac bypass surgery done by a female thoracic surgeon.
In this sense, I think the delicate nature of ophthalmic surgery—that is, in the public’s perception—has kept ophthalmology immune, so to speak, from the gender gap. It is almost shameful to share these thoughts, especially considering the gross stereotypes that have persisted in many societies for centuries.
In my career, ever since I have been a health care professional and a leader of a scientific team, everybody on my team is evaluated based on performance and abilities—never on gender. This is something that I believe, and I will not tolerate any exceptions.
I think that stereotypes in Europe, and Greece in particular, are stronger on the gender gap than they are in the United States, so more needs to be done to establish equality not just as a legality but also in society and education.
I am strict in conveying my personal beliefs to the rest of my team, and I am strict in creating a safe working environment for our female associates. We have a mechanism for reporting any offense or even the slightest suspicion that a visitor or patient will cross the strict line that we have set regarding harassment. I know from experience that putting strict rules in place and enforcing them is key to enjoying a gender-neutral working environment. Excelling in science and professional work requires us to employ rules and set strict guidelines so that no gender bias infects our daily routine.
Dr. Kılıç:
Yes, there are barriers to women’s advancement in ophthalmology. For starters, men’s salaries are higher than women’s. Also, there are more male heads of departments, presidents of societies, directors of eye clinics, speakers at conferences, and faculty at meetings. During scientific discussions, men are usually more active and sometimes even aggressive. When this is the case, women do not have an equal opportunity to join in these discussions. Many women feel hesitant or unable to jump into and interrupt scientific discussions among men. The mission, alongside our industry partners, in the editorial departments of journals, and at ophthalmology conventions, must be to boost awareness of equality issues such as these. (See more of Dr. Kılıç’s thoughts on industry collaborations in her accompanying sidebar.)
Advice for Women Who Wish to Work With Industry
Fruitful collaborations require improving your surgical skills, getting involved with innovations, and sharing your experience with colleagues.
By Aylin Kılıç, MD
I have been fortunate in my career to work with several of our ophthalmic industry partners in the development of innovative products. Each collaboration has a unique set of requirements, but at the core of the fruitful ones lies three tenets: improving your surgical skills, getting involved with innovations, and sharing your experience with colleagues.
After my residency, I started to work in a newly established private eye hospital. My challenge was to care for premium patients as a young doctor and simultaneously to increase my surgical experience. After 3 years, I was appointed as a director by the hospital and was responsible for overseeing 10 other ophthalmologists. I had the opportunity to perform thousands of cases while also educating other surgeons.
I was also traveling a lot, improving my skills and knowledge by attending international courses, meetings, and conferences. I was interested in academic work, too, continually writing articles and giving talks about some of the high-technology opportunities available at a private hospital that would not have been possible in refractive surgery at most universities.
Because of my publishing activity, the International Society of Refractive Surgery chose me to be a delegate from Turkey in 2008. I was the youngest and one of the few women ophthalmologists in this group at that time. I always attended their meetings, and that gave me good opportunities for international networking.
I was working on building my career, but at the time, I was using a different surname (Ertan). My status in private life changed in 2008, and I continued my career with Kılıç as my surname. That change has been a challenge for me and still is today because sometimes I am not recognized for my earlier work.
INVOLVED WITH INNOVATION
I have worked closely with different companies in the ophthalmic industry. In early relationships with industry, starting in 2006, my work was mainly related to helping companies educate surgeons about their products. Now, I am involved in multiple earlier-stage technologies.
For those interested in working with industry, there are a few important things to keep in mind. First, we always want to serve our patients the best we can. Therefore, it is valuable to improve our surgical skills, to be involved with innovations, and to share that experience with our colleagues.
I have always been interested in following new technologies, which means I have always wanted to be close to the industry. I feel a responsibility to give feedback to companies regarding clinical results with their new products. I want to explain how I use their products and how patients could benefit more from them if they were improved in certain ways.
My advice to everyone who desires to work closely with industry—not only women—is to participate as much as possible in international meetings, to collect your data and present it at conferences, and to publish articles. Contact companies to tell them about potential improvements and, more important, to give them feedback about how you use their product in your daily work.
REMEMBER YOUR ETHICAL RESPONSIBILITY
Remember that you must maintain your ethical responsibility for your patients. Especially for a new technology, always consider what would happen if this product were to be used by hundreds or thousands of surgeons around the world. Your voice is important; use it to guide the industry toward safe and effective solutions, and at the same time you can work to build your career.
Dr. McDonald:
There is still the perception that women with children, especially young children, are not able to take on extra tasks or responsibilities to advance their careers. This is not true. Female ophthalmologists who select supportive mates willing to make lifestyle adjustments so that their wives can advance their careers can certainly do just that.
In the past, many male doctors married nurses. This still occurs, of course, but a significant percentage of young male doctors now marry a female classmate. The relationship, while romantic, is also a true professional partnership, mutually supportive from the very beginning of the marriage.
Dr. Rau:
The largest disadvantage for women residents or ophthalmologists is that the heads of clinics are afraid that women will become pregnant and take extended leaves of absence—even very long leaves when they have more than one child. The fear is that maternity leave disrupts the continuity of their work in the clinic, and sometimes they choose to give up working in the clinic completely.
The other worry, for me as the head of a clinic, is when doctors who have small children must take time off to be with their children when they are ill. This means the head of the clinic must deal with giving more appointments to the remaining doctors, which means longer wait times for patients, overwork for the doctors, and a staff that is stressed by dealing with the patients who have those long wait times. (See more of Dr. Rau’s thoughts on owning her own private clinic in her accompanying sidebar.)
The Pleasures and Responsibilities of Practice Ownership
Making decisions and setting goals using my own expertise.
By Magda Rau, MD
I completed my medical studies and residency in the Czech Republic. Where I trained, the head of the eye department, Frydek-Mistek, Lydia Dolinova, MD, was very supportive, and I was able to start performing surgery early in addition to doing scientific work. After emigrating to Germany and working there for 2 years as a resident, I achieved recognition as an ophthalmologist there as well.
I was very fortunate with my place of residence because my chief professor, Dieter Dausch, MD, was a pioneer of excimer laser refractive surgery. In fact, he was the first to perform hyperopic excimer laser treatment.1 Dr. Dausch was my mentor in microsurgery and refractive surgery. I started to perform phacoemulsification, trauma and lid surgery, and excimer laser refractive surgery in Amberg and Nuremberg, Germany. My first scientific publications were made with him as coauthor. 2
MOVING TO PRIVATE PRACTICE
Later, I opened my own practice in a small German town, Furth im Wald, which also borders the Czech Republic. Even with all the daily work of maintaining the practice, I continued to participate in glaucoma clinical studies sponsored by companies in Europe and the United States.
I was one of the first surgeons in Germany to begin performing cataract surgery on an outpatient basis. I was also head of the eye department in the district hospital of Cham. Later, I transferred my outpatient surgery work to a clinic run by my husband, an anesthesiologist, also in Cham. In the beginning, other kinds of surgeries, such as orthopedic and gynecologic procedures, were also performed at that clinic. After my husband passed away, I changed the conception of the facility to be an eye clinic only.
DEVELOPING EXPERTISE
I began to develop expertise in multifocal IOLs, as I started to implant these devices when they were first introduced. I reported my results at international congresses, published, and gave instructional courses. To this day, I continue to add new multifocal and extended depth of focus IOLs to my spectrum of presbyopia-correcting offerings. I often combine different kinds of IOLs to answer the individual demands of patients.
In my experience with presbyopia-correcting IOLs, I have noticed a difference in the satisfaction rates between men and women. My studies have shown that women were more satisfied with higher-addition multifocal IOLs, most likely because they are not as tall as men, their arms are shorter, and they are more interested in finer details. Further, men felt limited by the worsening of distance vision with multifocal IOLs, which stems from their ancestry as hunters, because they like to have perfect distance vision. Additionally, they don’t like to hold reading material very close. I have reported about these results at congresses as well as in publications.
In addition to refractive surgery and IOL studies, I have taken part in glaucoma clinical studies (Refocus and Transcend). Augenklinik Cham was a part of the multicenter European study of the Cypass Micro-Stent (Alcon; no longer available). Our group and I have published and given presentations on these studies. My center was a reference center for Alcon representatives from all over the world who taught ophthalmologists the method for implanting the Cypass. Since its recall in 2018, I have moved to other MIGS devices, including the iStent inject (Glaukos) and the Omni Surgical System (Sight Sciences).
CONCLUSION
I appreciate being an owner of a private clinic because I can make decisions—medical, administrative, and organizational—using my own expertise. I can shape the goals of my own clinic. I am not responsible to a director of a hospital, and this allows me to introduce innovative methods without waiting for outside approval. It is my decision which equipment to buy, and it is my responsibility to pay for such tools—so practice ownership involves a mix of both advantages and disadvantages.
1. Dausch D, Smecka Z, Klein R, Schröder E, Kirchner S. Excimer laser photorefractive keratectomy for hyperopia. J Cataract Refract Surg. 1997;23(2):169-176.
2. Rau M, Dausch D. Intrastromal corneal ring implantation for the correction of myopia: 12-month follow-up. J Cataract Refract Surg. 2003;29(2):322-8.
Another possible behavior contributing to the gender gap is that individuals in leadership positions (ie, men) usually like to work with other men. And if women achieve good positions in an ophthalmology department or society, these women also usually prefer to work with men!
Professor Tassignon:
In government—in commissions for the evaluation of health care or pharmacology, for instance—there may not be enough women. It is not because there are not enough women on the faculty of medicine. Nowadays, it tends more to be 60% women and 40% men. Why don’t women apply? It’s often because they want to have their free time and their family time.
Dr. Visco:
I have encountered the same gender biases as a biology student, a bookkeeper, and a pharmacy technician as I encounter in ophthalmology. I will say that, today, the bias is much less and more subtle. The clearest way for women to become adept at overcoming bias is to practice whenever and wherever it’s encountered and as often as possible. In doing so, we hone our leadership talents and prepare for a bright future. A wise women once told me, “It can’t be that difficult if men do it all the time.” The change will come with time and with the development of more women in leadership roles.
5. What is the role of mentorship in a woman’s career journey? Spanning your career, which women have you looked up to? How have they influenced how you practice?
Dr. Arbisser:
Mentorship is a crucial part of everybody’s career journey, so I don’t know that it’s a gender issue. A mentor must be selfless, and it is therefore beneficial to have more than one mentor—it’s simply too much to ask one person to be great at what he or she does and be a full-time mentor to one or more people.
My mentors were my career mother and grandmother as well as my physician father and pediatric ophthalmologist husband, Amir. (Read more of Dr. Arbisser’s thoughts on mentorship in family in her accompanying sidebar.) In ophthalmology, when I was in medical school, John C. Nelson, MD, showed me the ropes, helping to cement my decision to enter the specialty. I then benefited from many surgeons, especially Howard V. Gimbel, MD; Randall J. Olsen, MD; and Steve Charles, MD, FACS, FICS. I also appreciate many industry representatives who recognized my talent and encouraged my ongoing curiosity and desire to be patient-centric.
Three Generations of Career Women and Counting
Why mentorship comes in many shapes, and how to make the most of an insight.
By Lisa Brothers Arbisser, MD
I have a unique perspective on mixing family and profession. My grandmother was a lawyer, and my mother was the psychologist, television personality, and columnist Dr. Joyce Brothers. It is pretty unusual to have three generations—and now four, including my son’s wife (daughter-in-love) who is a cantor and who with my son is raising our three grandchildren—of professional women. I had a head start in understanding the nuances of work-life balance, and, in every sense of the word, my mother and my grandmother were my very first mentors. They shared with me their knowledge, experiences, and advice—not about the profession of ophthalmology but rather about how to be a respected and successful professional and how to find the right balance in life between work and home.
Mentorship took another shape when I entered ophthalmology. I was only the second female resident ever to be accepted to the Department of Ophthalmology at the University of Iowa, and, at the time that I started practicing, very few of my colleagues were women. Some of the mentors I had—mostly men—were more virtual mentors in that I watched their surgeries but did not have a lot of one-on-one interactions with them.
But also, in those early days of my career, I was rather aggressive. Ophthalmic companies would invite me to join panel discussions, but some of my male colleagues refused to work with me. At one point, someone on the industry side approached me and offered me public speaking coaching so that I would come across as less aggressive. I could have taken that as a huge insult, but I decided to accept the offer. I really do believe that, if I had been a man, people would have considered me to be assertive, not aggressive (see Stereotypes and Double Standards in the Workplace).
That experience helped me to learn that one should not be wounded by small slights. Instead of being insulted by the offer, I took it as a well-meaning hint. It’s easy to be oversensitive about things, but taking a step back and looking at the big picture can sometimes be helpful and educational. Frankly, those individuals—mentors of a sort—helped me to become better at expressing my viewpoints more gently and constructively. It turned out to be useful advice in my career.
Now that I am retired from patient care, mentorship has taken a different shape: I am the mentor. One way that I try to stay both current and useful is by traveling to other ORs and watching my colleagues’ surgeries. That type of direct mentorship was not available to me when I was early in my career. I used to go to other people’s ORs, but they never came to mine. I hope to continue mentoring future generations of ophthalmologists for years to come.
Stereotypes and Double Standards in the Workplace
A Man Is…
- Assertive
- Direct
- Commanding
- Strong/Powerful
A Woman Is…
- Aggressive
- Shrill
- Pushy
- Domineering
Adapted from: Barriers and bias. American Association of University Women. https://www.aauw.org/app/uploads/2020/03/Barriers_and_Bias_summary.pdf. Accessed April 13, 2020.
Dr. BARSAM:
There are not too many high-volume refractive surgeons in the United Kingdom; however, early in my career, I was lucky enough to do a fellowship with Eric D. Donnenfeld, MD. During my time in the practice, I was able to observe and work with Dr. McDonald. I also think highly of Neda Shamie, MD; Beatrice Cochener-Lamard, MD, PhD; and Dr. Kılıç, all dynamic women I look up to and have learned from. These women have all the qualities that you would want in a refractive surgeon, irrespective of gender. They are caring, generous, motivated, dynamic, and experienced, and they work really hard.
Dr. Johansson:
I have looked up to many women in ophthalmology. In my country, there is one very apt surgeon and researcher in particular, Maria Kugelberg, MD, PhD, who I have worked with and whose work I continue to be aware of. We worked together only for a brief period, but she has been very successful in her scientific work and is a role model in many ways.
Dr. Kanellopoulos:
For many decades now, there have been great female clinicians, researchers, and educators who have contributed pivotal landmark and cornerstone advances in ophthalmology. One great example is Danièle Aron-Rosa, MD, PhD, the first person to perform Nd:YAG capsulotomy, a procedure that revolutionized postoperative cataract surgery care forever. Another equally great example is Dr. McDonald, the first person to perform an excimer laser ablation.
In my opinion, ophthalmology in the past few decades has had essentially no gender gap, as women and men alike are equal contributors to excellence in clinical care, research, and innovation. As a specialty, we are way ahead in bridging the gap in comparison to other specialties.
In my career, I had the opportunity to train in a residency program in New York led by the late Elsa K. Rahn, MD, an accomplished pediatric and strabismus specialist. Another outstanding mentor of mine was Deborah Pavan-Langston, MD, at Massachusetts Eye and Ear Infirmary in Boston, a world authority in cornea and herpetic disease. I also had a great retina surgery mentor in Pamela Ann Weber, MD, during my residency at the State University of New York, Stony Brook.
As I think it over, among the colleagues and peers I look up to, interact with, and learn from today, probably the same number are women as men. I am not sure I can say what unique perspective the female mentors that I had brought to me personally, as I never perceived a difference in any mentor based on gender. I have never, in my personal life, growing up with two sisters, nor in my professional career, had any predilection to consider a gender gap among colleagues or mentors.
Dr. Kılıç:
The role of mentorship is especially important for women’s careers. I have had both male and female mentors. Joseph Colin, MD, and Cynthia J. Roberts, PhD, each influenced my vision and my practice greatly. I admired Professor Roberts even before I met her because she was usually one of the few women on the panels at meetings and courses. She is always a strong contributor, and she has done a lot of valuable work in our field.
Dr. McDonald:
Mentors are important in anyone’s career. I was lucky enough to have a strong mentor for about 3 years, but my mentor was male. There were few female ophthalmologists when I started my career.
Dr. Rau:
Unfortunately, in my career, I have met only a few women who have supported me.
Professor Tassignon:
It is important to have mentors, people who are an example for you. Nowadays, young people think that their careers will be valuable only if they can study or practice at least 1 year abroad. It’s always good to visit other centers, but some people do it thinking that it will change their careers. I think that is wrong because they do it without the right perspective and goal. Go somewhere because you want to learn from that specific person, because that person can help you in your development or your thinking, not because it will improve your CV. This is the wrong attitude.
Make your choices carefully. That is, I think, the reason why congresses are still important. You can meet individuals, and you can get a sense of their philosophy. Does their way of thinking fit well with your way of thinking? Will the questions that come up be best answered by that person? (See more of Professor Tassignon’s thoughts on positive interactions with colleagues in her accompanying sidebar.)
The Life of an Inventor
Parallels with collegial collaborations.
By Marie-José Tassignon, MD, PhD, FEBO, FEBOS-CR
The gender gap is not something I have personally experienced. As a child, I engaged in typically girlish activities when playing with my sister and typically boyish activities when playing with my brother. I even played football on a boys’ team.
My training director at Brussels University was a woman and the first female university professor in ophthalmology in Belgium. She was very interested in surgery and introduced many new technologies to Belgium. When her binocular vision became poor, she asked me to take over her program in the OR. I was in my third year of training at the time.
A difficult period in my career occurred the year before she was due to retire. Jealousy was rampant among members of the ophthalmology team in Brussels, which was composed mainly of women. The inappropriate attitude of the director’s successor spurred me to leave Brussels University, and I applied for the chairmanship at Antwerp University. The total number of applicants for the position was 10, one woman and nine men. The faculty and the clinic jointly selected me. I was 38 years old when I took over as chair and chief of Antwerp Clinic and University in October 1991.
HEAVY INVOLVEMENT
Perhaps my experience has been an exception, but, apart from my application at Antwerp University, I have never applied for any position; rather, I have always been asked to apply. For example, Albert Galand, MD, PhD, asked me to apply for board membership in the ESCRS. Mary D’Ardis, as CEO and I, as a board member, were the only women. I became the organization’s first female general secretary in 1998 and the first female president when I served from 2004 to 2005. I then became the president of the European Board of Ophthalmology. Gisèle Soubrane, MD, was the first female president of the European Education Society. In 2007, Michael Blumenthal, MD, and José Barraquer, MD, nominated me to become a member of Academia Ophthalmology Internationalis, and I became the first female president of that society in 2019.
Combining a professional career with family life kept me extremely busy. My two children must have experienced many frustrations as a result, but they are following in my footsteps—both balancing careers and families and doing so successfully.
The life of an inventor follows much the same course as my own. You cannot apply to become an inventor; you become one by yourself but also thanks to the network you build over the years. Time—not your gender—will determine whether your invention will last. My mentors in patented inventions were male, but I have received tremendous support from both female and male ophthalmologists. These colleagues have supported me because they have understood my ideas and were not biased by their commitments to industry.
Dr. Visco:
Mentoring is a long-term relationship that focuses on the growth and development of the mentee. Mentoring is not coaching, which is also important, but rather it involves a finite relationship targeted at strengthening or eliminating a specific behavior. Mentors are very personal and help us see a destination without giving us specific instructions on the path to take. Coaches, on the other hand, tell us how to do things. I have had both mentors and coaches. Women also have role models where there is no personal relationship per se, but the role model has served to inspire us by breaking some glass ceilings.
I have many long-term and meaningful relationships inside and outside of ophthalmology with both women and men who have supported me as mentors, coaches, or role models. To begin naming them would risk forgetting someone. Everything I am and everything I have today are a compilation of my own thoughts and desires and the thoughts and desires of everyone who has influenced me. Basically, everything you see now bears some evidence of their influence.
6. As a woman, what do you think you bring to the table to mentor the future generation of ophthalmologists?
Dr. Arbisser:
Perhaps my example of longevity in teaching and my history of high-volume surgery while raising four children have served as positive models. One unique way I mentor people now that I have retired from patient care is to go into their ORs, by invitation, as a coach and observe their surgeries. Depending on the surgeon’s performance, I may or may not have anything to say during the surgery, but afterward we review the cases together. I take notes during the cases, and we go over things that I might’ve done differently with video and conversation.
Dr. Kılıç:
I am trying to work more with young ophthalmologists. Mentoring makes me more motivated about my own work because it allows me to discuss the work with these young people, and we share our experience with it. We can be more creative when we work as part of a team. Further, it makes me happy as I see their improvement, step by step.
Dr. McDonald:
I love being a mentor. I have learned a lot along the way that I am delighted to share with younger women—and with younger men. We are more alike than we are different!
Dr. Rau:
I think I serve as an example of how, even in clinics in small towns, you can take part in clinical studies, be innovative, work on new surgical methods, perform scientific work, publish scientific papers, and act as a reviewer for scientific ophthalmic magazines. I am also a board member of the non–peer-reviewed publications CRST Europe, Ophthalmology Management, and Ocular Surgery News.
Professor Tassignon:
As head of the department, I can provide a good overview of what is going on worldwide and connect trainees to people I know. A principle that is accepted now in quite a lot of European countries is to spend a couple of months or years training abroad. As a mentor, I give staff the opportunity to do that.
Also, I never think that I know everything. I teach trainees what I know; when that is done, and the person wants to go further, I send him or her somewhere else. That is what is most profitable for the candidate or for the staff as well as for the department where the person will work.
Dr. Visco:
I never considered that I would be someone who could influence future generations of ophthalmologists. My desire is simply to help others and share my excitement for my profession. I was always told as a child that hard work is the key to success, so I work hard at what I love. One of my greatest loves is learning, and my desire to share what I learn has taken me on the path I walk today.
7. How do you achieve a healthy work-life balance? Do you think this is different for women and men?
Dr. Arbisser:
I don’t know if anybody truly achieves a healthy work-life balance, but it is helpful to recognize that the definition of that is not only different for each person but also that it changes over time. Work-life balance looks different when you have an infant from when you have a toddler and then a teenager. It looks different when you are single from when you are married or in a committed relationship. It looks different depending on how committed you are to sports and friends. Work-life balance is constantly changing depending on the stage of life you are in.
I think, by and large, work-life balance is a lot easier for men to achieve than for women. Women tend to feel a great deal more responsibility for children than men because that’s been our culture for generations, not to mention that we’re the ones who have to be pregnant and nursing. I went to my oral boards with a breast pump. Learning to delegate appropriately is essential. You have to accommodate.
Dr. BARSAM:
It shouldn’t be different for women than men, but sometimes it is. I think everyone has their individual take on what work-life balance means. In my family, my wife is the main caregiver for our four children; however, that doesn’t mean that I don’t spend a significant amount of time with my family. For instance, I rarely do any clinical work on weekends unless I have an emergency, and I take time off from work around the holidays.
I try and be very responsible with the time that I give to being involved in congresses and conventions. Instead of traveling in a day or two before a congress, I’ll get to the destination the day of. I no longer spend 5 days attending conferences, although you obviously could. I do this to minimize my time away from the family and to balance my responsibilities.
Dr. Johansson:
I have always had activities outside of work. In the past, I spent a lot of free time singing in choirs. As I get older, I have been more restrictive in scheduling activities for myself outside of work, and this is because now I understand better the value of quality family time. I prefer to set aside time for family activities like sailing, skiing, and simply being with my young children. I have two sons, one 13 and one 16 years old. They both play instruments, and I like it when we play together and to hear them both at rehearsals and concerts.
I have children from my previous marriage, too, and when they were young they also played instruments, but I was not so good at following their activities. That’s a pity because I enjoy that very much now. It gives me a positive energy that I can carry into work.
When I look at my younger colleagues, there is much more equal sharing of the tasks that we have outside of our work compared to 20 years ago, and that is a good thing.
Dr. Kılıç:
I think there is no difference between women and men in this regard. I am happy with the balance I have between my private life and my work.
Dr. McDonald:
It’s a struggle to maintain a work-life balance. There are always publishing deadlines looming, slides to make, and a mountain of charts and IOL calculations to address. It helps enormously to get enough sleep and exercise. Most of all, it helps to have a great spouse or partner to help you stop and smell the flowers.
Dr. Rau:
Sometimes it is very difficult to maintain work-life balance. There is so much work to do between surgery, clinics, administration, and research. My approach is to make a schedule for my free time and force myself to keep to it. I have a Western horse and perform American dressage training and trail riding. If you have a horse, you must take care of it, so this makes it easier for me to justify my time away from the clinic.
I also try to stay in touch with my friends. I was a good tennis player in the Czech Republic, so I try to play tennis at least during my holidays. I also paint in my free time, and my other hobby is to go shopping and have fun with my girlfriends.
Leadership in a Crisis
Women political leaders have excelled at keeping the COVID-19 pandemic under control.
By Laura Straub, Editor-in-Chief
It’s impossible to turn on the television, read the news headlines, or even walk out your front door without being reminded of COVID-19. It is undoubtedly the most important and the most frightening global event in the world today. While we all turn to our political leaders for guidance, it’s natural to wonder who is guiding with grace and authority.
According to a recent article in Forbes,1 women political leaders are at the top of their game in the current crisis. The leaders of Germany, Taiwan, New Zealand, Iceland, Finland, and Norway are solid examples of how women have responded exceptionally well to the current pandemic.
In Germany, Chancellor Angela Merkel ensured that COVID-19 testing started almost immediately after the pandemic began—a fact that will likely help the country to loosen restrictions sooner than many other countries.2 Instead of putting Taiwan on lockdown, President Tsai Ing-wen introduced 124 alternative measures to block the spread of COVID-19. At press time, there had been only six deaths in the entire country.3
The number of COVID-19–related deaths is also low in New Zealand, at only 12.3 Prime Minister Jacinda Ardern enacted an early lockdown and mandated self-isolation of people entering the country soon after the first cases were reported on that island nation. Further, she’s ordered all returning New Zealanders to quarantine in designated locations for 14 days.
Iceland is poised to be the litmus test for the true spread and fatality rates associated with COVID-19, as Prime Minister Katrín Jakobsdóttir has made available to all its citizens free coronavirus testing.4 The country’s thorough tracking system has helped to ward off any lockdown orders and to keep its schools open. According to the Forbes< article,1 Iceland has screened five times as many individuals as South Korea.
In true millennial style, Finnish Prime Minister Sanna Marin has relied on social media influencers to spread fact-based information on the country’s strategies to manage the pandemic. More than 20 years Marin’s senior, Prime Minister Erna Solberg of Norway is also relying on nontraditional tactics to educate the public. She held a press conference for children only, during which she responded to their questions and explained why it was OK to be scared.5
“The empathy and care which all of these female leaders have communicated … who knew leaders could sound like this?” contributor Avivah Wittenberg-Cox wrote in the Forbes article.1 “There have been years of research timidly suggesting that women’s leadership styles might be different and beneficial. … It’s time we recognized it—and elected more of it.”
1. Wittenberg-Cox. A. What do countries with the best coronavirus responses have in common? Women leaders. Forbes. April 13, 2020. https://www.forbes.com/sites/avivahwittenbergcox/2020/04/13/what-do-countries-with-the-best-coronavirus-reponses-have-in-common-women-leaders/?fbclid=IwAR2j8fh3pS96m-jZ-qrmrHoBrXw9a1A9QLi_vZSGDyGtaT-aYNwej2R2RrA#20e0a8923dec. Accessed April 20, 2020.
2. German coronavirus curve gives reason for cautious hope. Reuters. April 9, 2020. https://uk.reuters.com/article/uk-health-coronavirus-germany-merkel/german-coronavirus-curve-gives-reason-for-cautious-hope-merkel-idUKKCN21R2FF. Accessed April 20, 2020.
3. COVID-19 Coronavirus Pandemic. Worldometer. https://www.worldometers.info/coronavirus/. Accessed April 20, 2020.
4. O’Grady S. A coronavirus test for anyone? In Iceland, it’s possible. Washington Post. April 2, 2020. https://www.pressdemocrat.com/news/10884442-181/a-coronavirus-test-for-anyone?sba=AAS. Accessed April 20, 2020.
5. Fouche G. Norway PM tells kids: ‘It is OK to feel scared’ during coronavirus. Reuters. March 16, 2020. https://www.reuters.com/article/us-health-coronavirus-norway-children/norway-pm-tells-kids-it-is-ok-to-feel-scared-during-coronavirus-idUSKBN2131NE. Accessed April 20, 2020.
Professor Tassignon:
For trainees in Belgium, listing hobbies strengthens their CVs because these people show that they can integrate easily into a social environment.
Work-life balance is indicative of how an individual copes with stress. That will differ between people, but not because of gender. It is often said that men are serial; they complete one task before moving on to another. Women are said to be more parallel workers—we are multitaskers.
Dr. Visco:
The duties of childrearing still fall mostly on the woman—and I don’t necessarily believe this is a bad thing. But as a result, women are more likely than men to take a break in their careers to raise children. There used to be a time when a woman had to choose one or the other; I chose both and had my children through medical school, residency, and early private practice. I had the advantage of having an amazing partner and supportive family to help. Today, families are getting more creative with their strategies, and my advice to women is to do whatever you want and not to apologize. We don’t balance work and life; there is no perfect plan or ratio. What you strive for is harmony and happiness regardless of the ratio. For me, this means letting go of perfectionism, actively learning to relax (ie, get an MBA degree … yes, this helped me relax!), exercise (not always easy), and structure your life as much as possible. (Read more of Dr. Visco’s thoughts on getting an MBA in her accompanying sidebar.)
Why I Got My MBA and Why More Women Should
I’m always trying to stay one step ahead of the game.
By Denise M. Visco, MD, MBA
Anyone who has been in a leadership position and experienced success will concur that leaders are not born, they are made. Leaders are made through the formal education process and through life experiences. Leaders are made through the nurturing and support of family and friends. Leaders are made through hard work, success and failure, and the ability to learn from mistakes.
At this point in my life, I am often congratulated on how much of a success I have made of myself, and it is truly a wonderful thing for the grandchild of an illiterate immigrant to be able to become a physician with a thriving practice. The elephant in the room for me is what it actually took to become what people see.
FOUNDATION FOR SUCCESS
I have worked hard and am still a very hard worker. I was taught first by my father that hard work and education are the foundations for success. I have always been interested in biology and the sciences, but my father, who was an accountant, insisted I have a basic grasp of accounting and economic principles. I took business electives in high school, participated and won state awards in Junior Achievement, and completed a Dale Carnegie scholarship before matriculating at the University of Delaware. During college, I held two part-time jobs, one as an accounts-payable manager for a small computer company and another as a pharmacy technician.
After my first year of college classes, I decided on and committed to attending medical school. I applied similar critical analytics when choosing my specialty and when opening a solo practice. After residency, I had several job offers that I rejected; instead, I chose to invest in myself. My calculations at that time indicated I would break even after 3 years of solo practice versus becoming an associate. By year 5, I would well surpass what anyone else would ever do for me. Those calculations turned out to be almost right.
OVERCOMING CHALLENGES
Over the past 25 years, I’ve had many challenges. Health care economics have been ever-evolving. It’s both difficult and stimulating to try to stay one step ahead of the game. I have made significant investments in expanding my practice and the services we offer. There have been times of great fear and times of great excitement. There have been many successes and some not so much. Failure is not an option, but it happens. With any new investment, there are the associated sunken costs of learning leadership.
My goal in pursuing an MBA a few years ago was first and foremost to be true to myself and my evolution as a leader. I am profoundly aware of how my decisions affect others, particularly in my practices. My MBA has enabled me to make better choices and see things from new perspectives. Furthermore, I have become more adept at articulating and communicating. I understand the importance of strategy, the impact of economics, and the nuances of change and crisis management. Although many physicians have administrators who perform their corporate functions, I am decidedly hands-on. I feel that it’s critical for physicians to make the business decisions in medicine. To advocate for patients, we need to engage the whole picture.
My clinic and ambulatory surgery center have invested heavily in our people. No one can be a leader without people who are willing to follow. Staff must be inspired through good times and bad. Value must be created in one’s vision. Respect must be garnered through honesty, integrity, and work ethic.
These are my goals as a leader today. I was not born with them; I acquired them. I highly recommend pursuing an MBA to fulfill your objectives in leadership, personal development, and business growth.
8. What barriers do women currently face in the profession that you feel are close to being broken down?
Dr. Arbisser:
Today, industry recognizes that, because their audience is more diverse, they need to have diversity on their advisory boards. The value of being an opinion leader is that you learn things sooner. You get different perspectives sooner. You see volume sooner. It’s also easier to be a patient advocate. It’s valuable to devote some of your time to industry work in order to be a better surgeon.
But, until you have the volume, industry is not so interested in you. And to get the volume, you have to be really, really good. And to be really, really good, you need to have knowledge of what equipment to use and how to use it. And to get the inside information on that, you almost need to be an opinion leader. So it’s circular. But I believe that it is easier to achieve these things today because industry understands that it’s to their benefit to have a diverse group of opinion leaders.
Dr. BARSAM:
There is a feeling that ophthalmology is a bit of an old boy’s club. At meetings, the makeup of panels and speaker programs may still be predominantly male. We know that there are equal numbers of females and males in medical school, so this shouldn’t be the case.
I’d love to see more diversity in ophthalmology. The gender gap will continue to shrink, but as long as it is still a male-dominated field, we will continue to see barriers. We’ve all got to work together to change this.
Dr. Kanellopoulos:
There is an unfair inequality for young female medical professionals who decide to proceed with starting a family. Women face all the difficulties that motherhood and bringing up young children can have on their professional careers. These manifestations of the gender gap have been well documented in many countries.
Greece is striving to be on par with other European Union countries, including the Scandinavian nations, to work toward an understanding that these factors are a fundamental and necessary part of life. We owe our female colleagues fairness in this regard. Nevertheless, barriers still exist, and working on them may eradicate them in the near future.
As a fortunate parent of two sons and a daughter, I think it is only fair that I—as all of us should—bring up my children without a gender gap and provide them with the possibility of achieving whatever goals they may set for themselves without barriers or stereotypes. This should be so in every aspect of professional life as well, including our environment of ophthalmology and ophthalmic care.
Dr. Kılıç:
This depends on the cultural and political situation. At some hospitals, there are still unfair differences in salaries and academic opportunities for women.
Dr. McDonald:
It is true that we still need more female leaders at the top, including department chairs, presidents of ophthalmic organizations, and award winners; however, we are getting more representation at the podium at meetings. That is a step forward.
Dr. Rau:
Unfortunately, I don’t think that the barriers will be broken down any time soon. Still, we have to do our part to work for this, with professional self-confidence that is based upon our expertise.
Professor Tassignon:
In Belgium, maternity leave is normally about 3.5 months. There are mechanisms built in now so that women can stay at home longer, but many don’t take it because they worry that their education will be longer, and it will take more time before they can work and earn money. They don’t claim the right because it’s not to their advantage. They take the same amount of time off as before the new policies were set. It is rare that women want to extend their maternity leave, but they are also helped much more by their partners today compared to even 10 or 20 years ago. The partner also takes part in raising the children.
Dr. Visco:
In ophthalmology over the past 5 years, I have seen more women on the podium and represented with industry. I think this is terrific, and the more conversations we have, the more gender bias will fade in other areas. We are getting there slowly. When equal female representation becomes the new expected norm, the condition will self-perpetuate.
1. Searing L. The big number: Women now outnumber men in medical schools. The Washington Post. December 23, 2019. https://www.washingtonpost.com/health/the-big-number-women-now-outnumber-men-in-medical-schools/2019/12/20/8b9eddea-2277-11ea-bed5-880264cc91a9_story.html. Accessed April 13, 2020.
2. Madigan JC. The education of girls and women in the United States: a
Historical Perspective. National Coalition of Girls’ Schools. 2009. https://www.ncgs.org/wp-content/uploads/2017/11/The-Education-of-Girls-and-Womenin-the-United-States-A-Historical-Perspective.pdf. Accessed April 21, 2020.
3. Graf N, Brown A, Patten E. The narrowing, but persistent, gender gap in pay. Pew Research Center. Available at: https://www.pewresearch.org/fact-tank/2019/03/22/gender-pay-gap-facts/. Accessed April 9, 2020.
4. Barriers & bias: the status of women in leadership. American Association of University Women. https://www.aauw.org/resources/research/barrier-bias/. Accessed April 9, 2020.
5. Gong D, Winn BJ, Beal CJ, et al. Gender differences in case volume among ophthalmology residents [published online ahead of print July 18, 2019]. JAMA Ophthalmol. doi:10.1001/jamaophthalmol.2019.2427.
6. La Roche J. Warren Buffett: women make me ‘very optimistic’ about this
country. Yahoo Finance. April 23, 2018. https://finance.yahoo.com/news/ warren-buffett-women-make-optimistic-country-120930431.html. AccessedApril 3, 2020.
7. Keller Johnson L. Exerting influence without authority. Harvard Business Review. February 28, 2008. https://hbr.org/2008/02/exerting-influence- without-aut. Accessed April 9, 2020.



