

The availability of SMILE has expanded the range of effective options we can offer to patients seeking refractive surgery to reduce their dependence on glasses. When I meet with patients who want refractive surgery, I try to understand their lifestyle and visual needs and recommend the refractive procedure that will best help them meet their visual goals.
My staff and I describe all refractive surgery options to patients and detail the differences between the procedures. Patients are usually already familiar with the LASIK procedure, but we usually have to educate them about PRK, SMILE, and phakic IOLs if one of them is the ideal option for the patient.
PROCEDURE AND INDICATIONS
The procedure. During the SMILE procedure, the VisuMax excimer laser (Carl Zeiss Meditec) creates a small incision and then a small disc-shaped lenticule of corneal tissue, which is removed from the eye to reshape the cornea. Research has demonstrated SMILE’s safety, efficacy, predictability,1,2 and excellent visual outcomes.3 Because most of the anterior tissue remains intact, corneas exhibit less biomechanical weakening after SMILE than after LASIK.4,5 Furthermore, fewer superficial corneal nerves are severed during SMILE (Figure), which reduces the risk of postoperative dry eye symptoms.6,7
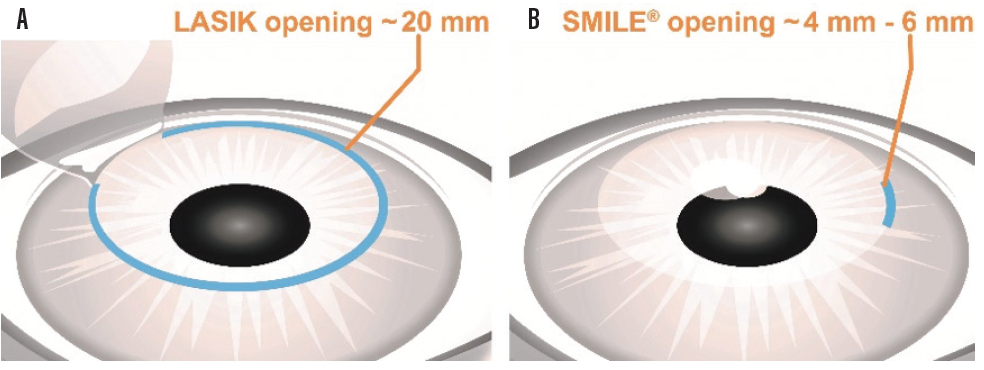
Figure. Comparison of LASIK (A) and SMILE (B) incisions.
Indications. SMILE patients must have appropriate corneal thicknesses, healthy topographies, and reasonable tear dynamics.8 I recommend starting with patients who have at least -3.00 D of myopia because the lenticule is thicker and more resilient during removal. With experience, surgeons become comfortable performing the procedure in lower dioptric ranges.
RECOMMENDING THE IDEAL REFRACTIVE PROCEDURE
In my current use, if patients fall within -2.00 to -10.00 D of myopia with astigmatism less than -3.00 D, I tend to recommend SMILE. This is especially true if they are involved in contact or extreme sports (which are common in the area I practice in). When patients with those hobbies ask me about LASIK, I point out it is also a great procedure but I would recommend that we proceed with SMILE. I often then help them understand that, if they move during the first 8 seconds of the SMILE procedure, I will probably convert to LASIK anyway. Essentially all of my patients have been comfortable with this explanation.
For appropriate candidates, I recommend LASIK as the primary procedure. In my practice, this includes patients with myopia below -2.00 D, astigmatism above -3.00 D, or hyperopia.9 I tend to perform PRK or phakic IOL implantation if the residual stromal bed thickness would be a close call with LASIK or when I think patient compliance would make it difficult to complete SMILE or a LASIK flap.
I have found that verbally preparing patients for what they will see and feel during the procedure helps to keep them relaxed and makes them less likely to move while the suction is engaged. With the VisuMax system, the suction is low enough that patients can still see the flashing target beam during the procedure; this makes it much easier for them. I also verbally talk them through the time that the suction is engaged, and I have found that it makes a profound difference in their compliance. If an enhancement is necessary at some later date, I either perform PRK or convert the SMILE cap into a LASIK flap.
CONCLUSION
When clinical guidelines are followed, SMILE is an excellent surgical choice for the right candidate. In the future, indications will likely expand to include hyperopia.
SMILE: A Refractive Surgery Option for Thin Corneas
By Jay Bansal, MD
A 35-year-old man presented to our practice seeking refractive surgery. His refraction had been stable for 3 years, and he was otherwise healthy. He wore toric contact lenses, which we instructed him to discontinue for 3 weeks before laser vision correction surgery.
His preoperative manifest refraction was -7.25 +2.75 x 82° = 20/20- OD and -7.25 +3.00 x 96° = 20/20- OS. Central corneal thickness was 531 µm OD and 523 µm OS. Corneal topography showed normal, symmetric astigmatism (Figure 1). Belin-Ambrósio analysis on Pentacam (Oculus Optikgeräte) Scheimpflug imaging revealed D values of 2.17 OD and 2.08 OS (Figure 2).
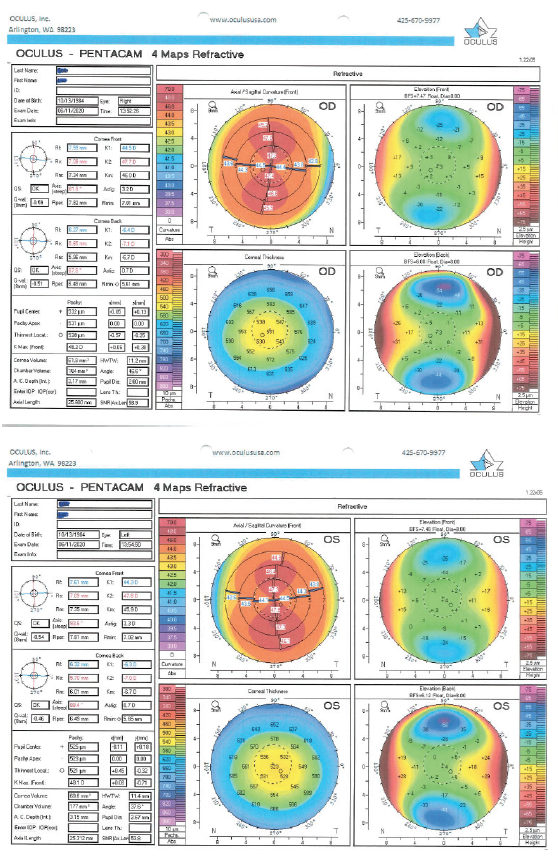
Figure 1. Preoperative corneal topography.
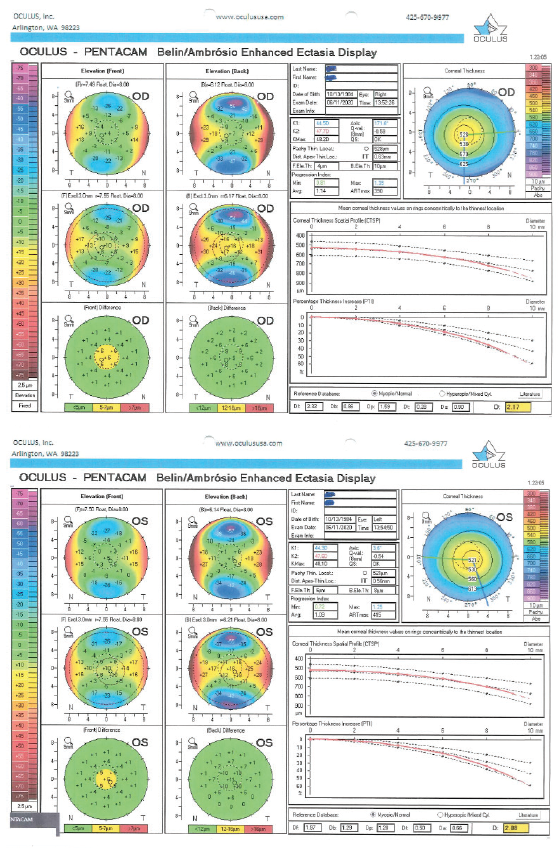
Figure 2. Preoperative Belin-Ambrósio enhanced ectasia analysis.
Because the patient had high myopia and high cylinder and his corneas were relatively thin for this particular refraction, I opted to perform SMILE rather than femtosecond LASIK (femto-LASIK). During this flapless procedure, the VisuMax femtosecond laser (Carl Zeiss Meditec) creates a circular corneal lenticule that is surgically removed. The process flattens the central corneal curvature to correct the patient’s refraction.
Research has shown that SMILE results in less biomechanical weakening of the cornea than femto-LASIK. Wu et al found that SMILE protected the cornea’s structural integrity, with less disruption of the peripheral collagen fibers than femto-LASIK.1 Patients with high myopia within approved indications who have SMILE rather than femto-LASIK may be at less risk of corneal ectasia after surgery. Additionally, it is reported that patients have less postoperative dry eye and fewer flap complications with SMILE because it does not involve creation of a flap or the use of photoablation.2 My personal experience reflects this finding as well.
At the 2-month postoperative visit, this patient’s UCVA was 20/20- OD and 20/25 OS.
Conclusion
Although femto-LASIK and SMILE have similar indications and contraindications, I prefer SMILE to treat patients with high myopia, thin corneas, moderately steep corneas, and/or mild ocular surface disease, within approved indications.
1. Wu D, Wang Y, Zhang L, Wei S, Tang X. Corneal biomechanical effects: small-incision lenticule extraction versus femtosecond laser-assisted laser in situ keratomileusis. J Cataract Refract Surg. 2014;40(6):954-962.
2. Denoyer A, Landman E, Trinh L, Faure JF, Auclin F, Baudouin C. Dry eye disease after refractive surgery: comparative outcomes of small incision lenticule extraction versus LASIK. Ophthalmology. 2015;122(4):669-676.
1. Hansen RS, Lyhne N, Grauslund J, Vestergaard AH. Small-incision lenticule extraction (SMILE): outcomes of 722 eyes treated for myopia and myopic astigmatism. Graefes Arch Clin Exp Ophthalmol. 2016;254(2):399-405.
2. Blum M, Taubig K, Gruhn C, Sekundo W, Kunert KS. Five-year results of small incision lenticule extraction (ReLEx SMILE). Br J Ophthalmol. 2016;100(9):1192-1195.
3. Sia RK, Ryan DS, Beydoun H, et al. Visual outcomes after SMILE from the first-year experience at a U.S. military refractive surgery center and comparison with PRK and LASIK outcomes. J Cataract Refract Surg. 2020;46(7):995-1002.
4. Wu D, Wang Y, Zhang L, Wei S, Tang X. Corneal biomechanical effects: small-incision lenticule extraction versus femtosecond laser-assisted laser in situ keratomileusis. J Cataract Refract Surg. 2014;40(6):954-962.
5. Seven I, Vahdati A, Pedersen IB, et al. Contralateral eye comparison of SMILE and flap-based corneal refractive surgery: computational analysis of biomechanical impact. J Refract Surg. 2017;33:7:444-453.
6. Denoyer A, Landman E, Trinh L, Faure JF, Auclin F, Baudouin C. Dry eye disease after refractive surgery: comparative outcomes of small incision lenticule extraction versus LASIK. Ophthalmology. 2015;122(4):669-676.
7. Cai WT, Liu QY, Ren CD, et al. Dry eye and corneal sensitivity after small incision lenticule extraction and femtosecond laser-assisted in situ keratomileusis: a meta-analysis. Int J Ophthalmol. 2017;10(4):632-638.
8. VisuMax Femtosecond Laser. Small incision lenticule extraction (SMILE) procedure for the correction of myopia. Professional use information. Accessed August 17, 2020. https://www.accessdata.fda.gov/cdrh_docs/pdf15/P150040D.pdf
9. Reinstein DZ, Pradhan KR, Carp GI, et al. Small incision lenticule extraction for hyperopia: 3-month refractive and visual outcomes. J Refract Surg. 2019;35(1):24-30.
