

The landscape of refractive surgery has changed immensely since the first excimer laser procedures were performed in the early 1990s. Today, in addition to femtosecond LASIK and PRK, patients have the opportunity to select from other corneal laser refractive surgery procedures, including SMILE, and even lens-based surgical options including refractive lens exchange, refractive cataract surgery, and phakic IOL implantation. Having this variety of procedures available helps us to expand the indications for refractive surgery and to increase the number of patients who are candidates for these elective procedures. We can finally select the best procedure for every unique patient.
As a refractive surgeon, I perform both lens- and cornea-based refractive surgical corrections, and the indications I use for each type of procedure have expanded or changed over the years. This article focuses on my indications for phakic IOLs.
EXPANDING INDICATIONS
Until 2015, I used a classical pathway of patient selection for phakic IOL surgery with the EVO Visian ICL (STAAR Surgical) in my clinic. Most patients were younger than 50 years of age and had myopia of -6.00 D or more, pachymetry readings of less than 470 μm, suspicious topography, or low residual stromal bed thickness. All other patients with less than -6.00 D of myopia underwent laser vision correction (LVC), assuming they were good candidates for cornea-based procedures.
Today, my indications for phakic IOLs are broader, and I implant the EVO Visian ICL in patients with low (< -3.00 D) or moderate (< -6.00 D) myopia with the following conditions:
- All objective and/or subjective symptoms of dry eye disease;
- Risk factors for retinal detachment (eg, younger presbyopic myopic patients without a posterior vitreous detachment;
- High regular astigmatism (> -3.00 D); or
- Low residual stromal bed thickness.
I will also implant the EVO Visian ICL by the patient’s choice as a removable surgical option that presents no contraindications for future refractive procedures because it preserves the cornea. Further, I prefer the ICL in patients with large pupils because it requires less ablation and a smaller transition zone than LVC procedures. Lastly, I will suggest phakic IOL implantation for patients who desire a quick visual recovery, especially if PRK is the only other option because more comfortable laser techniques are less suitable.
In Europe, the EVO Visian ICL is indicated in phakic patients between the ages of 21 and 60 years with up to -20.00 D of myopia and up to 6.00 D of astigmatism and in patients between the ages of 21 and 45 years to correct up to 16.00 D of hyperopia and up to 6.00 D of astigmatism.
PREOPERATIVE EVALUATION IS KEY
A careful preoperative evaluation is the key to successful postoperative results with the EVO Visian ICL, as is sound clinical judgement. It is crucial, therefore, that the surgeon consider the risk-to-benefit ratio before counseling patients that phakic IOLs are the right option. Individuals with an anterior chamber depth of less than 2.8 mm or with an anterior chamber angle less than grade 3 are not good candidates for this surgery, for example.
Another important part of the preoperative evaluation is helping patients to determine for themselves which procedure is the best option for them. In my opinion, greater emphasis should be placed on the responsibility shared between patients and health professionals in surgical decision-making. It should not be solely up to the surgeon to decide. Discussing the pros and cons of the procedure, even when patients have already made up their minds, and reviewing the safety information with them during the preoperative counseling process is mandatory. The pros and cons of the procedure that I outline for my patients are listed in the accompanying sidebar.
Today, refractive surgery patients are already well informed when they step into a practice. Some patients ask specifically for a phakic IOL, so I always explain the benefits of this technology as a part of the options.
GROWING THE SEGMENT
Changing the organization of our practice to give patients the option of both lens- and laser-based techniques has promoted tremendous growth in our practice’s refractive surgery numbers. In the past, using more traditional indications and targeting patients with high myopia only for phakic IOL surgery, the practice was performing an average of 111 EVO Visian ICL procedures annually. Only 9% of those procedures were for the indication of low myopia. In the 5 years since we started expanding indications to include patients with low and moderate myopia, our numbers have grown. Of the more then 300 EVO Visian ICL procedures we performed in 2019, 20% were for the indication of low myopia.
By offering both surgical procedures, we even expanded the group of LVCs by 9% in our practice. This is important because happy patients are the best advertisement for a practice.
Postoperative results in phakic IOL patients are typically excellent, and patients are happy with their surgical outcomes. In our practice, word-of-mouth referrals constitute 70% of our patients. It also helps that patients feel a part of the decision-making process—this strengthens their level of satisfaction with the procedure.
PROS AND CONS OF PHAKIC IOLS
Pros
- Safety and predictability
- Removability
- Decreased risk of dry eye disease compared with laser vision correction
- Quicker visual recovery compared with PRK
- Can be performed as immediately sequential bilateral implantations
- No contraindications for future refractive surgery
Cons
- The routine risks of any intraocular procedure
- Financial choices relating to the cost of the lens
- Any limiting factors with occupation or hobbies (eg, combat sports)
CONCLUSION
With so many refractive surgery procedures to choose from today, patients must understand the advantages and disadvantages of each, and they must be educated on the importance of selecting the right procedure for their own eyes. When the proper clinical indications are considered, there is no doubt that patients will typically be satisfied with their postoperative results.
Refractive Surgery in a Keratoconic Eye: Phakic IOLs Were the Best Fit
By Andrea Russo, MD

The demand for refractive surgery increased in my practice after the COVID-19 lockdown. One of the reasons for this rebound effect is our patients’ need to wear masks during the pandemic. The consequent fogging of glasses experienced by many patients has inspired them to seek refractive surgery.
Interestingly, many of these patients had previously undergone a refractive surgery evaluation and were found not to be good candidates for reasons including keratoconus or ectasia risk, thin corneas, high prescriptions, or tear disorders. Many of these patients are candidates for phakic IOLs, and these are the ones now expressing the greatest preoperative enthusiasm and postoperative satisfaction. The only drawback for me with this group of patients is removing their “inoperable” label, therefore contradicting the previous opinion they had received from another ophthalmologist.
I recently counseled a patient with keratoconus who desired refractive correction. After a detailed conversation (see the sections Advantages of Phakic IOLs and Addressing Concerns), we decided that phakic IOL implantation was the best chance this patient had to achieve spectacle independence.
ADVANTAGES OF PHAKIC IOLS
At least here in Italy, most patients are aware only of laser vision correction (LVC) as a refractive surgical option. The idea of a lens inside their eye is therefore frightening at the beginning. In these cases, I spend extra time explaining the procedure and highlighting the advantages of the EVO Visian ICL (STAAR Surgical) over LVC.
In particular, I show an animation of the procedure, available from Rendia. During the video, I describe the positioning of the ICL behind the iris, and I explain that the procedure is fast, usually taking no more than 5 minutes per eye. I note that the recovery time is comparable to, if not faster than, recovery from LASIK.
ADDRESSING CONCERNS
Still, one of the main concerns expressed by patients is the presence of a lens inside the eye. “What if I rub my eyes, or if something hits the eye?” I reassure them that these lenses are not rigid but rather extremely soft, and they can go back to their normal lives with confidence. I add that ICLs are routinely implanted in US Army personnel, a further guarantee of their quality and safety, and I mention the potential reversibility of the procedure.
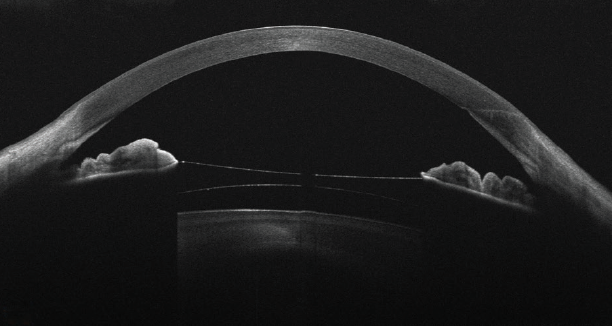
Figure. Representative OCT scan of an eye with keratoconus implanted with an ICL.
It is often noted that LVC is less invasive than phakic IOL implantation. Particularly for this group of patients, however, I sometimes consider a reversible and upgradable phakic IOL to be less invasive than a definitive laser treatment—especially for a patient who would be left with minimal residual stromal thickness not allowing future enhancements.
Further, I am often asked by young patients, “What if my prescription changes over time?” Our eyes are living organs, and we can never be sure about the stability of an individual’s prescription, especially those with medium to high myopia. This is why I prefer phakic IOLs, which leave all the surgical options on the table for the future if a prescription changes. This flexibility is met with a sigh of relief from my patients.
AN EXCELLENT OUTCOME
In the case of the keratoconus patient mentioned at the outset of this article, CXL was first performed to stabilize the ectasia. After following the patient for 12 months and confirming corneal stability, a toric ICL was implanted. The resultant postoperative visual acuity was 20/20, and the patient was extremely happy with his outcome.
