



Nearly anyone you ask will say that they have heard of LASIK. Many of them will even use the term for any type of surgical vision correction—and for good reason. Over the past 25+ years, LASIK has been the most commonly performed procedure for surgical vision correction, and its volume is growing. In 2020 alone, at the height of the COVID-19 pandemic, more than 630,000 refractive procedures were performed, the majority of them LASIK. The Refractive Surgery Council predicts that 2021 will have the highest volume of refractive procedures performed since the Great Recession.
What about the future of refractive surgery? First, this specialty is no longer limited to LASIK but includes newer options for laser vision correction (LVC) and lens-based surgery. Additionally, patients with presbyopia, a condition that affects approximately one-third of US adults, have been underserved historically. The research and development of new procedures and technology, however, is improving surgeons’ ability to treat this population. Lastly, cataract surgery, once a purely medical procedure, now can provide some patients with the best vision of their lives.
WHAT’S NEW IN LVC?
The safety and results of LASIK have never been better, and LASIK is not the same procedure it was 25 years ago. It is the most studied medical procedure and has even been dubbed the “most successful, elective procedure.”1 Studies have shown that, on average, visual acuity and the incidence of dry eye are better after LASIK than with glasses or contact lenses.2,3
The development of procedures such as SMILE and technologies such as Contoura Vision (Alcon) and iDesign Refractive Studio (Johnson & Johnson Vision) has increased the number of treatment options and the level of customization that surgeons can offer to patients. SMILE, approved by the FDA in 2016, is the newest and fastest-growing form of LVC on the market. This flapless procedure achieves visual results similar to those of LASIK but with fewer flap/cap complications and less (and temporary) postoperative dryness and discomfort (Figure 1).4 Topography-guided LASIK with the Contoura, also approved in 2016, can achieve visual results that were not previously possible.5 The iDesign, approved in 2019, has iteratively improved the visual outcomes achieved with wavefront-guided LASIK.6
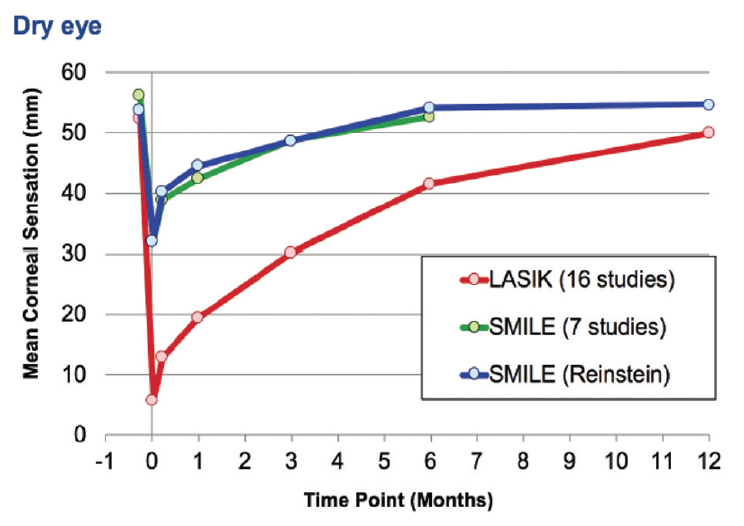
Figure 1. The incidence of dry eye after LASIK and after SMILE at various postoperative timepoints.
Courtesy of Dan Z. Reinstein, MD, MA(Cantab), FRCSC, DABO, FRCOphth, FEBO
WHAT’S THE FUTURE OF LVC?
Affordability and fear are the reasons most commonly given by patients who are interested in but do not undergo surgical vision correction. Demographics are another factor, but the LVC industry is growing despite these hurdles (Figure 2).
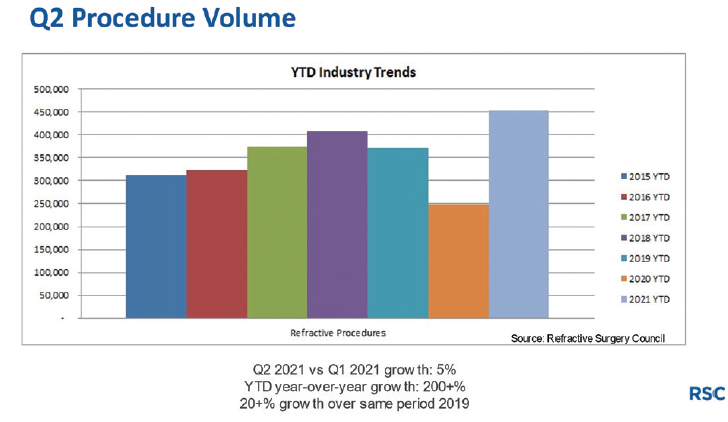
Figure 2. Refractive industry trends.
Improved affordability. On average, LVC costs 15% less today than it did in 2008.7 Further, financing companies such as CareCredit, Alphaeon Credit, and GreenSky offer subscription models that can make surgery more affordable for patients.
Diminished fear. I find fear to be the greatest deterrent for people interested in surgical vision correction. Despite the excellent safety profile of LVC, nearly every patient I encounter can cite the procedure’s risks, including dry eye, night vision concerns, and flap-related complications. For many people, perception is reality. I therefore expect that technologies that offer a perceived risk reduction—like a flapless procedure such as SMILE or, when it is available in the United States, the corneal lenticule extraction for advanced refractive correction procedure (CLEAR, Ziemer)—will grow the LVC market (Figures 3 and 4).
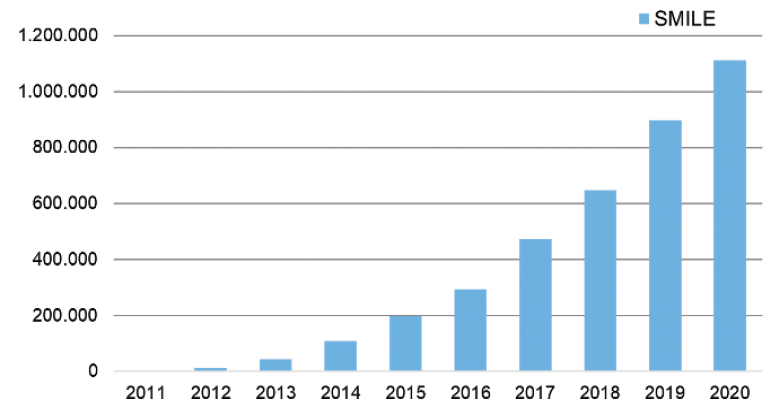
Figure 3. Worldwide SMILE volume.
Figures 2 and 3 courtesy of the American Refractive Surgery Council
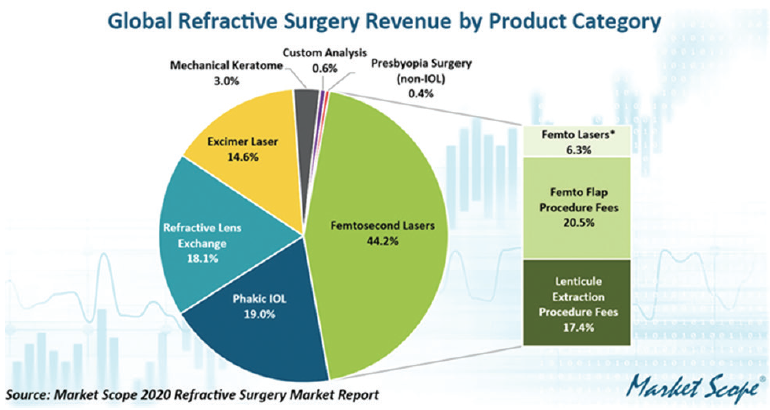
Figure 4. Global refractive surgery revenue.
Demographics. Millennials, now the largest generation group in the United States, are becoming financially independent, with salaries that allow many of them to afford refractive correction. This prospective pool of candidates should generate an increase in the number of refractive procedures for years to come. Some members of Generation Z are also now old enough to benefit from vision correction, and I find that many of them seem to be interested in the newest forms of LVC.
WHAT’S NEW IN LENS-BASED CORRECTION?
Phakic IOLs. This form of refractive correction has significant growth potential. The Visian ICL (STAAR Surgical) is the only phakic IOL approved in the United States, and it is the market leader worldwide (Figure 4). In the United States, the market for the ICL has been much smaller than elsewhere in the world. This IOL is often considered to be an option only for highly myopic patients or those with thin or abnormal corneas. The available power range and sizes of the ICL, however, are expanding, and astigmatism is now an approved indication.
The largest barrier to widespread adoption of this lens is currently the requirement for a peripheral iridotomy (PI). Outside the United States, a version of the ICL with a hole in its center, the Evo ICL, is available. This lens eliminates the need for a PI. The size of its optic is also larger. It is to be hoped that this model will become available in the United States in the near future.
The latest Market Scope data estimates that ICL implantation in the United States will constitute 11.1% of all refractive procedures within 3 years. In addition to the easing of safety concerns related to the requirement of a PI with ICL implantation, surgeons can now perform the procedure in an in-office surgery suite safely and cost-effectively.8,9 The removability of this lens can make it more appealing than an ablative procedure for some patients.
Premium IOLs. The premium IOL market is exploding, and many patients choose to undergo refractive lens exchange (RLE) for vision correction (discussed in further detail later).
PRESBYOPIA: THE NEWEST AND FASTEST-GROWING FRONTIER
The surgical correction of presbyopia has grown over the past 5 years to represent almost 50% of my surgical volume, and I expect procedural volume to continue to increase.
Blended vision. This procedure continues to be a solid option for patients with presbyopia who are not ready for a lens-based option. Iterative improvements such as presbyopic LASIK are expected to reduce anisometropia by extending depth of focus.
Refractive lens exchange. Many patients over 40 years of age present to my practice with a desire to recover the range of vision they once had. Most of these patients are willing to pay for RLE. They are also one generation away from their parents, who are enjoying great vision after refractive cataract surgery, and they want that same quality of vision for themselves.
Extended depth of focus phakic IOLs. In the more distant future, extended depth of focus phakic IOLs will be an option for patients with presbyopia. These lenses may be a good fit for individuals who are not interested in RLE and those who wish to improve their visual acuity after cataract surgery.
Refractive cataract surgery. Most cataract surgeons will say that cataract surgery is refractive surgery, even when standard monofocal IOLs are used. A strong argument for optimizing the refractive result of cataract surgery is that readers and bifocal glasses have been associated with an increased risk for falls in the elderly.10 Based on patient demand and diminishing reimbursement rates for cataract surgery, I believe that a growing number of cataract surgeons will focus more on the refractive aspect of cataract surgery. Thankfully, current premium IOLs provide a greater depth of focus with fewer dysphotopsias than earlier models. Further, technology such as the Light Adjustable Lens (RxSight) can make refractive targets easier to hit. The volume of premium IOLs implanted is on the rise, and I anticipate further increases (Figure 5).
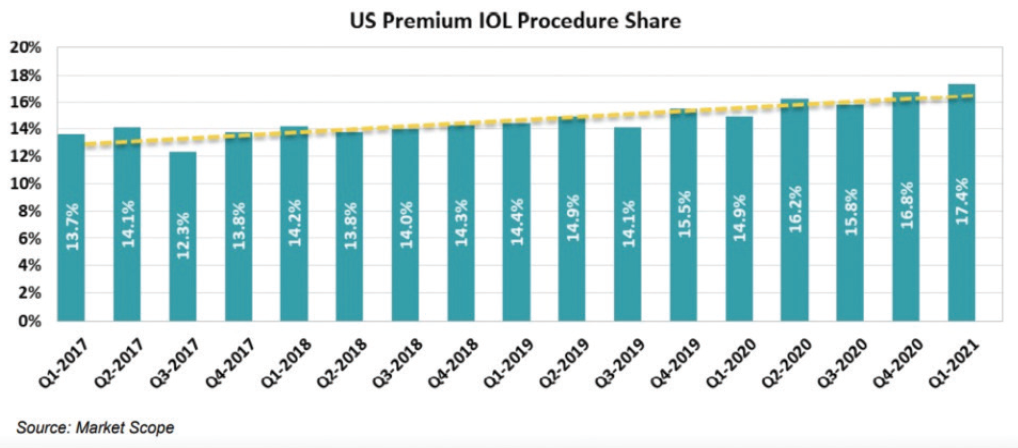
Figure 5. Premium IOL procedure share.
Figures 4 and 5 courtesy of Market Scope
Presbyopia drops. Significant progress has been made with topical drops that either increase depth of focus through pinhole optics or increase accommodation through a softening of the crystalline lens. It is expected that most of these drops will be prescribed by optometrists. Some surgeons are concerned that drops will reduce the need for refractive surgery, but I anticipate that many patients will need to undergo the surgical correction of ametropia to achieve optimal vision. Further, presbyopia drops will likely be a gateway to surgical methods for vision correction as patients become more aware of medical and surgical options for presbyopia correction.
CONCLUSION
The distant future of refractive correction is difficult to predict. Any technology that increases safety, improves visual outcomes, and personalizes treatment will likely grow the market. I am keeping my eye on the following:
- Laser-induced refractive index change, with its greater safety compared to incisional procedures and improved personalization after IOL placement; and
- Gemini Refractive Capsule (Omega Ophthalmics), with its potential for future versatility.
It is an exciting time to be a refractive surgeon.
1. LASIK called safest, most successful elective procedure in the world. Healio. November 10, 2017. Accessed August 13, 2021. https://www.healio.com/news/ophthalmology/20171110/lasik-called-safest-most-successful-elective-procedure-in-the-world
2. Eydelman M, Hilmantel G, Tarver ME, et al. Symptoms and satisfaction of patients in the Patient-Reported Outcomes With Laser In Situ Keratomileusis (PROWL) studies. JAMA Ophthalmol. 2017;135(1):13-22.
3. Price MO, Price DA, Bucci FA, Durrie DS, Bond WI, Price FW. Three-year longitudinal survey comparing visual satisfaction with LASIK and contact lenses. Ophthalmology. 2016;123(8):1659-1666.
4. Han T, Xu Y, Han X, et al. Three-year outcomes of small incision lenticule extraction (SMILE) and femtosecond laser-assisted laser in situ keratomileusis (FS-LASIK) for myopia and myopic astigmatism. Br J Ophthalmol. 2019;103(4):565-568.
5. Durrie D, Stulting DR, Potvin R, Petznick A. More eyes with 20/10 distance visual acuity at 12 months versus 3 months in a topography-guided excimer laser trial: Possible contributing factors. J Cataract Refract Surg. 2019;45(5):595-600.
6. Schallhorn SC, Venter JA, Hannah SJ, Hettinger KA. Outcomes of wavefront-guided laser in situ keratomileusis using a new-generation Hartmann-Shack aberrometer in patients with high myopia. J Cataract Refract Surg. 2015;41(9):1810-1819.
7. LASIK isn’t as expensive as you might think. American Refractive Surgery Council. October 29, 2018. Accessed August 13, 2021. https://americanrefractivesurgerycouncil.org/lasik-isnt-as-expensive-as-you-might-think/#:~:text=In%202008%2C%20the%20cost%20of,10%2Dyear%20period%20to%20%2422.50
8. Ianchulev T, Litoff D, Ellinger D, Stiverson K, Packer M. Office-based cataract surgery: population health outcomes study of more than 21 000 cases in the United States. Ophthalmology. 2016;123(4):723-728.
9. Enhance your practice with office-based cataract surgery. iOR Partners. Accessed August 30, 2021. https://iorpartners.com/office-based-surgery/
10. Chang DH. Multifocal spectacle and monovision treatment of presbyopia and falls in the elderly. J Refract Surg. 2021;37(S1):S12-S16.
