
Current techniques for cortex removal in cataract surgery rely on the aspiration of the cortex once it has been separated from the capsule. Successful aspiration is achieved when the outward centrifugal countertraction from the lens capsule and zonules is greater than the inward centripetal forces needed to break the adhesions between the capsule and lens fibers. Removing cortex is therefore more challenging in eyes with weak or absent zonules because the available centrifugal countertraction is reduced.
The primary surgical approach to removing cortex in eyes with weak or absent zonules is pulling the cortex centrally and relying on countertraction from either the remaining zonules outside the capsular bag or an implanted device inside the capsule, such as a capsular tension ring (CTR) or capsular tension segment.
A novel technique that eliminates the need for capsule countertraction from other sources is to inject OVD into the plane between the cortex and capsule to separate the layers and push the lens capsule and cortex away from each other.
THE TECHNIQUE
Cortical cleaving viscodissection involves filling the anterior chamber with OVD, separating the anterior and posterior lens fibers from the lens capsule, and separating the stronger equatorial lens cortex adhesions. Separation of the equatorial cortex is usually unsuccessful if the adjacent anterior or posterior lens fibers are still attached to the capsule. (Watch a video demonstration of the cortical cleaving viscodissection technique below.)
Step No. 1: Filling the anterior chamber with OVD. This creates a higher-viscosity environment, which helps keep the anatomical structures of the eye in their desired positions, reduces the flow rate to prevent rapid changes in IOP, and deepens the anterior chamber to increase the distance between the lens capsule and vitreous and the corneal incision and to act as a barrier between them.
Step No. 2: Viscodissection of the anterior lens cortex from the lens capsule. The cannula is introduced between the lens capsule and the anterior cortical fibers, and OVD is injected to propagate a wave of viscodissection to overcome the adhesions between the two. If an opening between the lens cortex and capsule does not already exist, the cannula tip can be used with gentle blunt dissection to create the initial plane between them (Figure 1). Once this plane is identified, injection of OVD is used for viscodissection of the anterior cortical fibers.
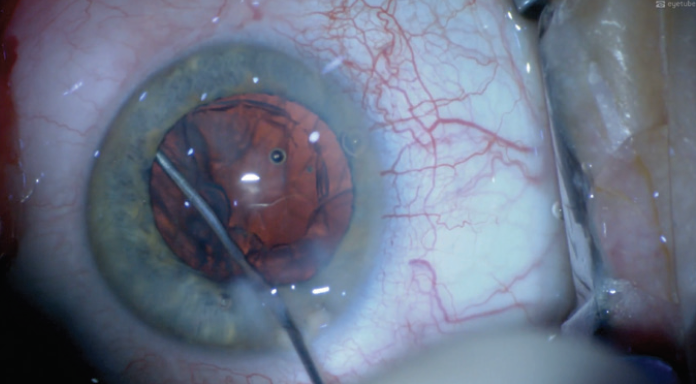
Figure 1. Gentle blunt dissection with a cannula tip creates the initial plane between the lens cortex and capsule.
The aim is to extend the dissection of the anterior lens fibers off the lens capsule and out to the equator of the lens. Achieving the desired direction of injection is important. For the areas of the lens capsule closer to the incision, a curved cannula can be used (Figure 2). A straight or curved cannula, depending on ergonomics, can be used to access the quadrants to either side of the corneal incision.
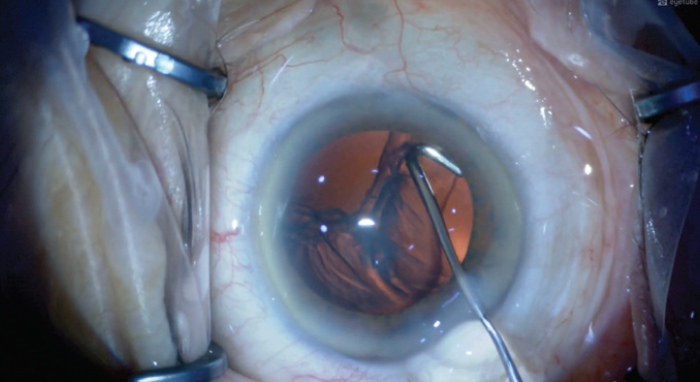
Figure 2. A curved cannula is used for viscodissection of the anterior lens fibers near the corneal incision.
Step No. 3: Viscodissection of the posterior lens cortex from the lens capsule. An opening in the posterior lens fibers can be created with the tip of the cannula using gentle blunt dissection at a shallow angle. Once an opening is present, viscodissection is used to break the adhesions in the plane between the lens fibers and capsule in an increasing area out to the equator of the lens (Figure 3). If there is cortex next to an already bared area of the lens capsule, the viscodissection plane can sometimes be created with an OVD injection alone, eliminating the need for blunt dissection.
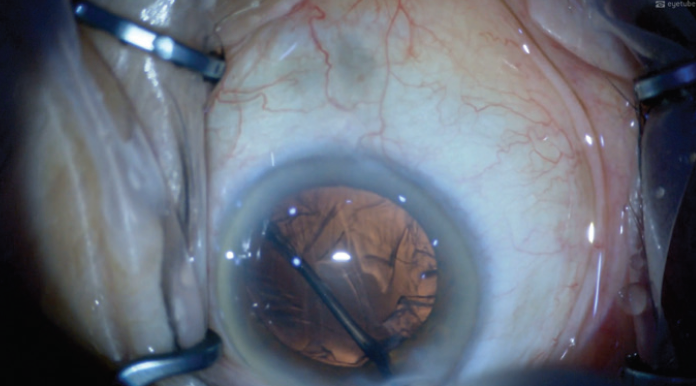
Figure 3. Viscodissection of the posterior lens cortex from the lens capsule is performed.
Step No. 4: Viscodissection of the lens fibers from the lens equator. Separation of the lens cortex from the lens capsule is most difficult to achieve in the fornix of the lens. This is where the corticocapsular adhesions are the strongest, and they rarely separate unless both the anterior and posterior segments of the lens fibers have already been viscodissected. Once the equatorial adhesions have been successfully viscodissected, the cortex separates from the capsule and moves away from the lens equator. A characteristic arc of tissue can then be seen against the red reflex (Figure 4).
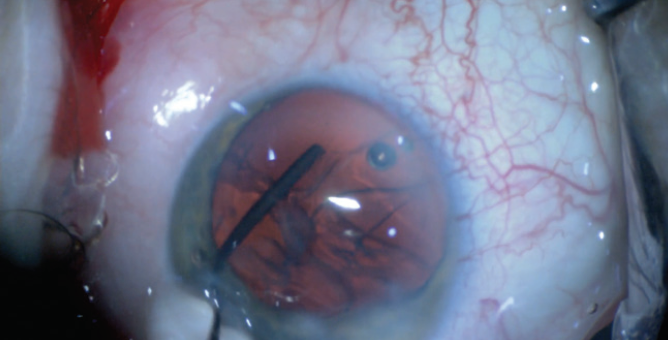
Figure 4. The free cortex is visible against the red reflex.
In my experience, an OVD injection directed radially from a location close to the fornix of the lens equator is most effective, and an anterior-to-posterior direction of injection is easier to achieve. Sometimes, repeated viscodissection from in front of and behind the lens fornix is required to free the adhesions in this area.
Step No. 5: Removal of free cortex from the eye. Opening the corneal incision by pressing on its posterior surface with a cannula will allow the slow, controlled removal of free cortex from the eye (Figure 5). Sometimes, the injection of more OVD between the capsule and free cortex is required to create a pressure gradient.
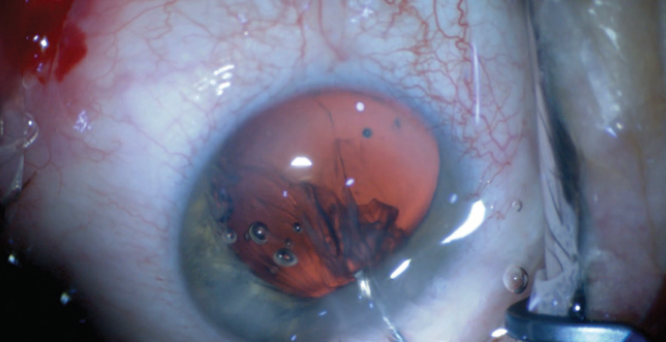
Figure 5. Pressure is placed on the corneal incision to allow slow, controlled removal of free cortex from the eye.
With this technique, the cortex can be removed entirely without the need for irrigation and aspiration, leaving the lens capsule filled with OVD and ready for CTR or IOL insertion. The expected volume of OVD needed to complete this technique is 2.0 to 4.0 mL.
INDICATIONS and ADVANTAGES
Indications. Cortical cleaving viscodissection can be useful in any case in which zonules are absent or abnormal, tractional forces on the zonules would be preferably avoided, or other techniques would be difficult or unsafe.
Avoiding zonular traction during cataract surgery is necessary in eyes with weak or absent zonules and desirable in eyes with pseudoexfoliation and previous blunt trauma and in which weak zonules can be anticipated. This alternative approach to cortex removal is also applicable to patients with stiff cortical cataracts, which are resistant to hydrodissection; when intraoperative floppy iris syndrome or posterior capsular rupture occurs; and when only peripheral lens cortex remains because it can be difficult to achieve aspiration with limited remaining anterior lens fibers.
Advantages. Keeping the anterior segment filled with OVD and having only OVD infused is beneficial because it keeps flow levels low, causes only slow changes in IOP, allows the surgeon to manually control IOP and alter the flow rate instantaneously, prevents rapid movements of intraocular tissues, creates a barrier to the forward movement of vitreous, traps lens particles, and allows instruments to be passed through the corneal incisions without rapid IOP changes. Additionally, stopping the infusion does not lead to globe decompression, and its direction of introduction is controlled. The opposite of all these can be true when balanced salt solution infusion is used to maintain anterior segment inflation.
Focal capsule-stabilizing devices that connect the capsule to the outer corneoscleral coat of the eye such as capsular hooks or capsular tension segments provide stronger countertraction to capsule retropulsion than lens equatorial centripetal forces, and cortical removal remains difficult with their use. CTRs provide lens equatorial countertraction, but they can also trap cortex between the IOL and lens capsule, making cortex removal more challenging even when a modified Henderson CTR (Morcher) is used. Placement of a CTR external to lens cortex can be achieved if OVD has been injected between 360º of anterior cortical fibers and the capsule. This is not, however, reliably achieved because the CTR could penetrate between cortical fibers at the lens equator at any point during insertion. One study using Miyake-Apple video analysis found greater displacement and torque of the lens capsule with early CTR placement, suggesting that CTR placement into an empty lens capsule is safer.1
A theoretical advantage of the technique is that, without using traction on the lens capsule, further damage to already weakened or compromised lens zonules can be avoided. Further, the technique may decrease the likelihood of late bag and lens dislocation. Cortical cleaving viscodissection can also be used for cortex removal without the need for CTR countertraction, allowing CTR insertion to be delayed until after the cortex has been removed.
CONCLUSION
Cortical cleaving viscodissection uses standard ophthalmic OR consumables and straightforward intraocular maneuvers that produce slow movements of the lens particles. The technique therefore can be reliably performed by an experienced surgeon even in challenging situations.
1. Ahmed II, Cionni RJ, Kranemann C, Crandall AS. Optimal timing of capsule tension ring implantation: Mikake-Apple video analysis. J Cataract Refract Surg. 2005;31:1809-1813.
