


I began implanting the IC-8 small-aperture IOL (AcuFocus) in eyes with irregular corneas 3 years ago. The design is based on the pinhole effect achieved with the Kamra corneal inlay (CorneaGen). The IOL was originally designed as an extended depth of focus solution to presbyopia. For me, however, the IC-8’s niche is for the treatment of irregular corneas because the implant can eliminate aberrations and improve quality of vision. In eyes with irregular astigmatism, the implant’s embedded mask blocks peripheral aberrated light rays and prevents them from degrading image quality, and the collimating effect of the central aperture provides a focused image. When a patient with a history of radial keratotomy (RK) presents for cataract surgery, my thoughts immediately turn to the IC-8.
Achieving excellent UCVA after cataract surgery is more difficult in patients with irregular corneal astigmatism. It is challenging to obtain accurate preoperative measurements of eyes with keratoconus, corneal scars, or a history of RK. I find helping these patients, however, to be especially satisfying, and it has become a special interest of mine. This article shares three cases in which implantation of the IC-8 led to a successful outcome and provides advice on implementing the technology based on my experience (see Ten Tips for Success).
Ten Tips for Success
1. OPTIMIZE THE HEALTH OF THE OCULAR SURFACE
Keratometry measurements to calculate IOL power are required even for eyes with irregular corneas. Maximize the health of the tear film and the ocular surface to get the most accurate measurements possible.
2. OBTAIN MULTIPLE MEASUREMENTS
Measure irregular corneas with multiple devices. The integrated keratometry function of the Barrett Universal suite of formulas can be helpful when there is no single perfect measurement of corneal shape. Taking a mean or median of the measurements with various devices can reduce the chance of error in an eye with an irregular cornea.
3. ACCOUNT FOR A HYPEROPIC SHIFT
Patients with a history of radial keratotomy (RK) often experience a hyperopic shift over time. Consider targeting a mildly myopic outcome during cataract surgery to compensate.
4. PLACE INCISIONS CAREFULLY
When operating on post-RK eyes, try to make the main incision between the RK incisions to prevent them from opening. Because the incision through which an IC-8 (AcuFocus) is implanted is large (2.75–3.5 mm), it may be impossible to avoid the RK incisions in some eyes. In this situation, consider making a scleral incision and avoid cutting the cornea completely.
5. MAINTAIN A CLEAR OPTICAL ZONE
Strive to keep the optical zone central to the opaque ring of the IC-8 clear. Polish the capsule and completely remove OVD from behind the IOL. If required, an Nd:YAG laser capsulotomy can be performed. I am conservative and prefer to perform the Nd:YAG treatment outside rather than inside the opaque ring because I want to avoid lens pitting.
6. ADDRESS REGULAR ASTIGMATISM
Some eyes have a high degree of regular astigmatism, and a toric model of the IC-8 is not currently available. In this situation, I recommend implanting the IC-8 in the capsular bag. After an accurate postoperative subjective refraction is obtained, a supplemental toric IOL can be implanted in the sulcus.
7. BE AWARE OF PUPIL SIZE
In some eyes, the outside diameter of the IC-8’s opaque ring is smaller than the pupillary diameter, so light can come around the outside of the opacity. This has not caused a problem in my experience. I have successfully implanted the IC-8 in young patients with large pupils.
8. CHECK ALIGNMENT
In my experience, the IC-8 centers well within the capsular bag. I have had no cases in which normal physiologic decentration caused visual side effects. I use the reflections of the operating microscope to check that the IOL center aligns with reflections corresponding to the corneal vertex because this is a good indication of the visual axis.
9. INFORM PATIENTS OF WHAT TO EXPECT
Explain to patients that the IOL can cause dimming. If they will receive an IC-8 in only one eye, counsel patients to expect some difference in brightness between their eyes. I have not had a patient who felt that the trade-off was not worth the improved vision. One of my patients who underwent bilateral implantation of the IOL, however, found the dimming noticeable when driving at night.
10. ASSESS VISUAL POTENTIAL
A trial with a rigid gas permeable contact lens can be a great way of assessing the visual potential of an eye with irregular astigmatism. If there is a significant improvement over the spectacle refraction, then the implantation of an IC-8 is likely to be beneficial. Of course, a trial is not possible in the setting of cataract opacity.
CASE EXAMPLE NO. 1
Presentation. A 63-year-old woman was referred to me for a cataract surgery evaluation by her optometrist. The patient was experiencing a reduction in the BCVA of her left eye. She had progressive myopia and variable refractive astigmatism in both eyes.
The patient had undergone bilateral RK for myopia 20 years earlier followed by astigmatic keratotomies for residual astigmatism, and she received hyperopic LASIK 10 years later. She was understandably hesitant about further surgical intervention. We therefore decided to treat the left eye first and assess her quality of vision before deciding on the treatment for her right eye. On examination, her uncorrected distance visual acuity (UDVA) was 6/48 OS, and her BCVA was a poor-quality 6/24 OS. Ten radial, near–full-thickness RK incisions approaching the visual axis; more peripheral astigmatic keratotomy scars; and a peripheral, circumferential LASIK scar were evident in each cornea. A moderately dense nuclear sclerotic cataract and an early posterior subcapsular cataract had developed in each eye (Figure 1).
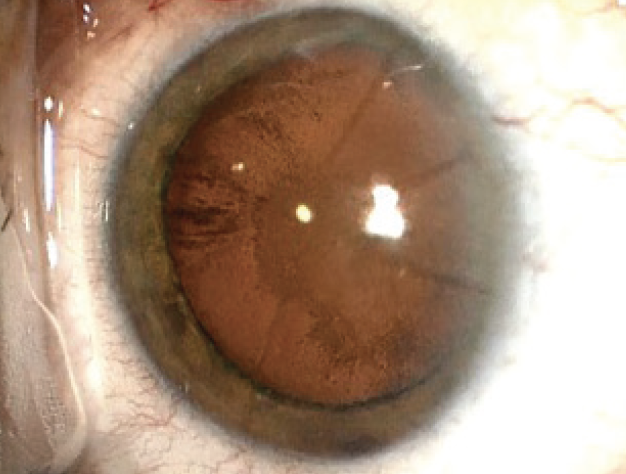
Figure 1. Intraoperative view of RK scars and cataract in Case No. 1.
The posterior segment of both eyes was healthy. As expected, the anterior keratometry measurements varied widely between devices. The readings, however, also varied when multiple measurements were obtained with the same device. After several attempts to optimize the health of the ocular surface, the patient returned for repeat keratometry, which showed marked diurnal variation. This is a typical finding in post-RK eyes. Corneal tomography (Figure 2) displayed irregular corneal astigmatism, as expected.
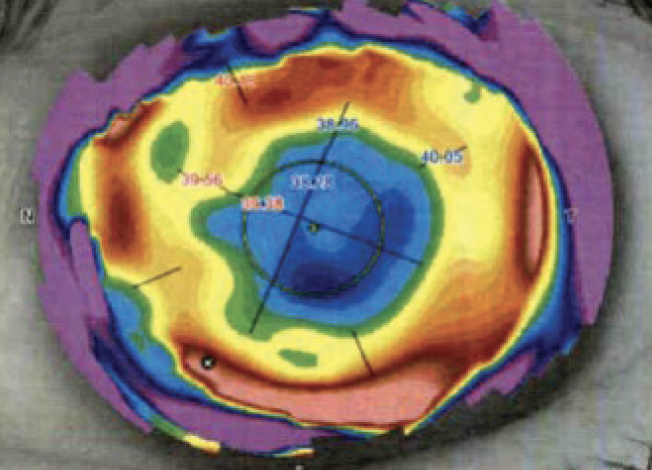
Figure 2. Anterior corneal topography showing irregular astigmatism.
Surgical considerations. Given the patient’s history of RK and LASIK, I wished to avoid further corneal ablation. Topography-guided phototherapeutic keratectomy is an excellent and safe method for regularizing corneal shape in many situations.1 The patient’s history of corneal refractive surgery, however, raised the risks of variable preoperative measurements and postoperative inflammation. Both the magnitude and axis of the astigmatism varied, rendering planning for a toric IOL imprecise. Moreover, the irregular nature of the astigmatism made it unlikely that a toric IOL would provide a satisfactory solution in terms of vision quality.
The patient and I discussed the pros and cons of implanting an IC-8. I explained the difficulty of performing an accurate IOL power calculation on her eyes owing to her history of multiple refractive procedures. She decided to proceed with cataract surgery and the implantation of an IC-8 in the left eye.
A gradual and ongoing hyperopic shift is expected in eyes that have undergone RK, so I aimed for a moderately myopic postoperative refraction. Surgery was without complication (Figure 3).
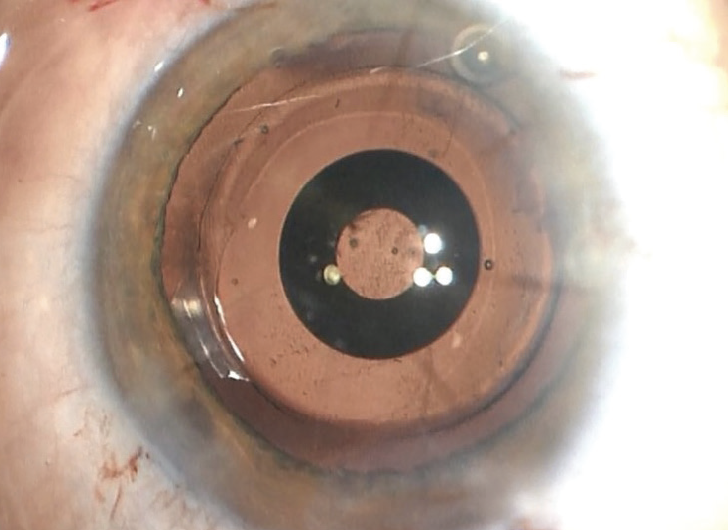
Figure 3. The IC-8 IOL in situ.
Outcome. The patient experienced an immediate improvement in vision after surgery. At 1 month, her UDVA was 6/6, and she could read N6 comfortably unaided. We were both happy with the outcome, and she subsequently underwent similar surgery on the contralateral eye.
CASE EXAMPLE NO. 2
Presentation. A 40-year-old woman referred to me for an evaluation was experiencing an intolerable fluctuation in vision throughout the day despite having a healthy ocular surface. She had undergone RK surgery overseas.
The patient’s UDVA was 6/6 OD and 6/24 OS. Her BCVA with spectacles was 6/12 OS with a lot of glare. Her BCVA with a rigid gas permeable contact lens was 6/7.5 OS, but she could not tolerate long-term wear of the contact lens.
The left eye had six RK incisions and one arcuate incision in the midperipheral cornea (Figure 4). The subjective refraction was highly variable.
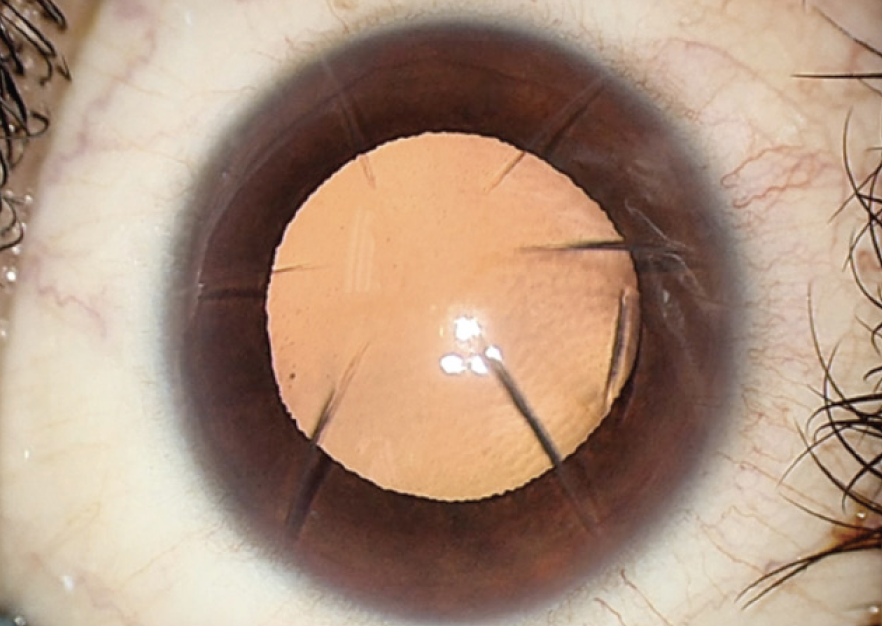
Figure 4. Preoperative view of the corneal incisions in case No. 2.
Surgical considerations. Corneal topography measurements were too inconsistent to proceed with a keratorefractive laser procedure. With glasses, contact lenses, and keratorefractive laser treatment ruled out, the best option for the patient was intraocular surgery. I have two main concerns with refractive lens exchange in eyes like this. First, the surgery would render the young eye instantly presbyopic. Diffractive multifocal technology would not be appropriate behind such an aberrated cornea, making a monofocal IOL the only option. Second, eyes with previous RK are usually highly myopic. The patient’s eye was therefore at increased risk of retinal detachment because it had not yet experienced a posterior vitreous detachment.
The patient elected to receive an IC-8 IOL to reduce diurnal fluctuations in vision, improve vision quality, and provide some depth of focus.
Surgery was straightforward. Rather than the manufacturer-recommended 3.5-mm incision, the IOL was implanted through a 2.75-mm incision, which sealed with hydration alone (Figure 5). I find that the smaller incision reduces surgically induced astigmatism and allows better prediction of refractive outcomes. The IC-8 comes with its own injector, but I prefer to use a standard Monarch III IOL Delivery System (Alcon; Figure 6).
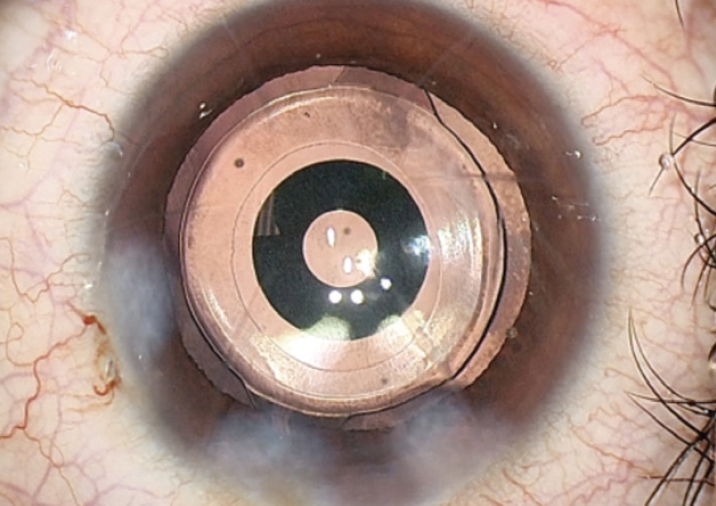
Figure 5. An IC-8 IOL implanted through a 2.75-mm incision, which sealed with hydration alone.
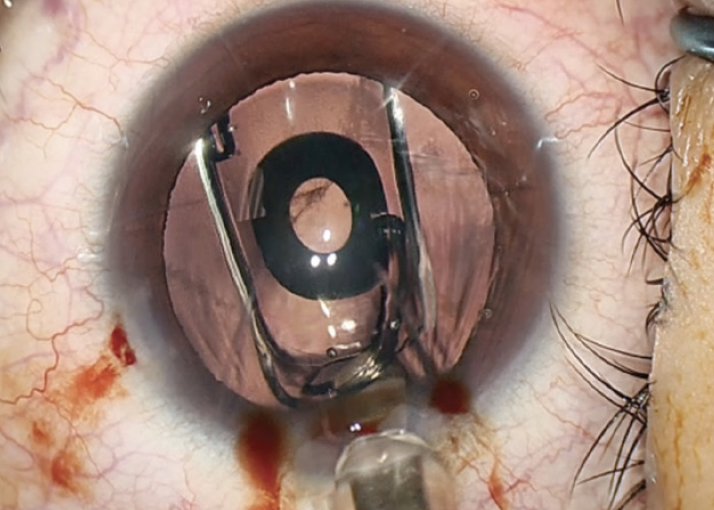
Figure 6. Injection of an IC-8 with a Monarch III IOL Delivery System.
Outcome. One year after surgery, the patient’s UCVA was 6/6. A concern when implanting an IOL in only one eye of an individual who is not presbyopic is whether the patient will tolerate the loss of accommodation in the implanted eye. In my experience, patients seem to tolerate this change with an IC-8 IOL better than with other IOL technologies.
CASE EXAMPLE NO. 3
Presentation. A 73-year-old woman with bilateral keratoconus was referred for cataract surgery. The corneal ectasia had been stable for many years, but the patient had developed a significant cataract and experienced a myopic shift in each eye.
Surgical considerations. The right eye had relatively regular corneal astigmatism, so a monofocal toric IOL was implanted with a distance target. The central cornea of the left eye was severely irregular, and the patient’s BCVA was 6/15 OS. In my experience, if the BCVA is poor with spherocylindrical spectacle correction, then a toric IOL is unlikely to provide an optimal visual outcome.
Topography-guided laser ablation was performed to regularize the cornea. A central 1-mm optical zone was used to minimize tissue loss, and a wide transition zone was used to minimize unwanted optical side effects (Figure 7). After surgery, the patient’s BCVA was 6/7.5, but her quality of vision remained suboptimal.
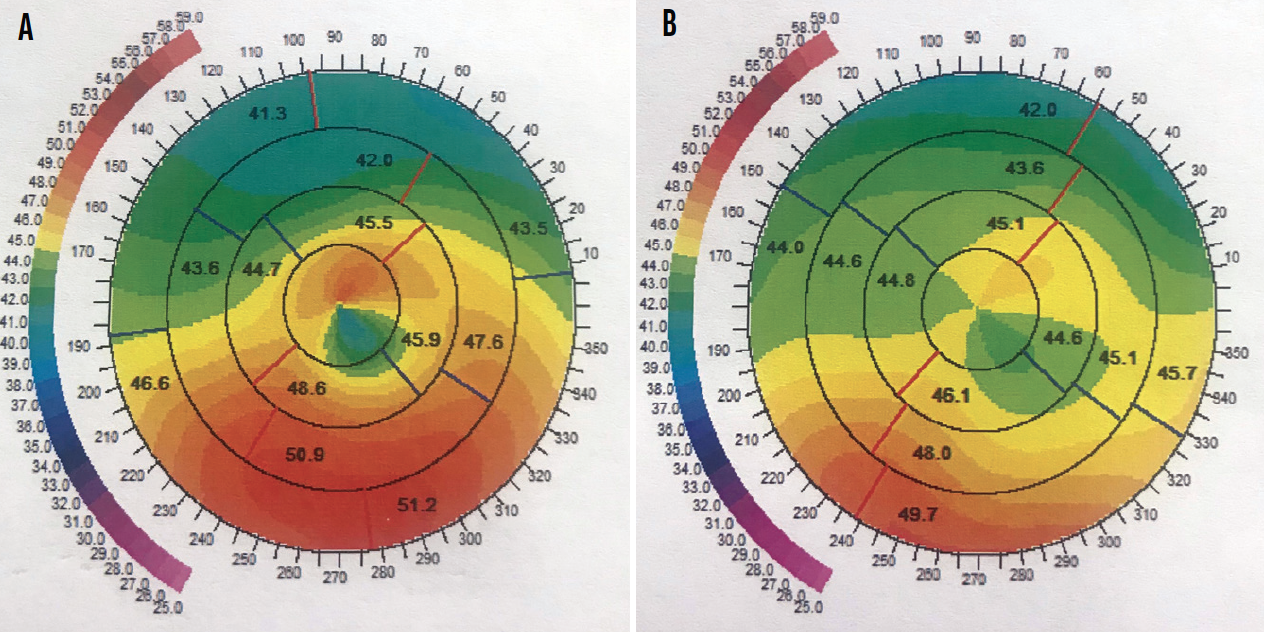
Figure 7. Before (A) and after (B) topography-guided laser ablation to regularize the central cornea of the eye in Case No. 3.
I had an extensive discussion with the patient, and she elected to undergo the implantation of an IC-8.
Surgical considerations. The patient’s left eye was nondominant, and she was keen to be independent of glasses. I therefore targeted mild myopia with the expectation that the IC-8 would provide an extended range of vision.
The capsule was polished to minimize the chance that posterior capsular opacification would affect the central optical zone. After implantation of the IC-8, the OVD was thoroughly aspirated from behind the IOL (Figure 8).
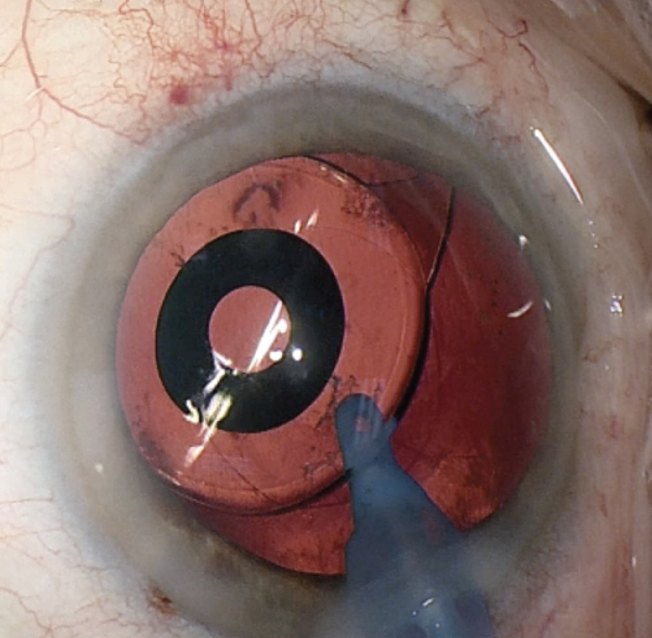
Figure 8. OVD is removed from behind the IOL.
Outcome. The patient was thrilled to be able to read fine print after surgery. Her quality of vision improved owing to a reduction in higher-order aberrations.
DISCUSSION
A growing number of patients with a history of RK are presenting for cataract surgery. I find that the IC-8 IOL offers two major benefits for this population.2 First, these individuals tend to tolerate a wide range of spherical refractive outcomes because of their depth of focus. Small residual refractive errors due to inconsistent preoperative measurements or a hyperopic shift generally do not prevent good visual outcomes. Second, patients can achieve an excellent quality of vision with up to 1.50 D of uncorrected astigmatism because the pinhole optics absorb this error.
I usually favor trifocal and extended range of vision IOLs when trying to achieve spectacle independence in patients with regular corneas. I view the IC-8 as a therapeutic option for patients with irregular corneas.3 The visual aberrations induced by traditional multifocal IOLs can compound preexisting aberrations from an irregular cornea. I therefore avoid the technology in this situation.
The IC-8 is an effective solution for presbyopia,4 but the potential for slightly dimmer vision postoperatively must be discussed with patients before surgery.5 Noticeable dimness has not been reported with bilateral therapeutic implantation of the IOL. Moreover, the IOL has been shown to have no effect on visual field testing, and retinal imaging and surgery may be safely performed via the view through the IC-8.
A thorough preoperative discussion with patients is required before implanting an IC-8 IOL for the treatment of corneal irregularities. Discussing the pros and cons of each lens takes time, but it allows both the patient and me to ensure that our goals and expectations are in sync. This is especially important when multiple surgical procedures are planned.
Any ophthalmologist who would like to discuss a case in which the use of an IC-8 might be appropriate is welcome to contact me directly.
1. LaHood BR, Goggin M, Ryan TG, Beheregaray S. Topography-guided transepithelial phototherapeutic keratectomy to treat a partial laser in situ keratomileusis flap amputation over the visual axis. Journal of Cataract and Refractive Surgery Online Case Report. 2019;7(3):33-35.
2. Agarwal S, Thornell EM. Cataract surgery with a small-aperture intraocular lens after previous corneal refractive surgery: visual outcomes and spectacle independence. J Cataract Refract Surg. 2018;44(9):1150-1154.
3. Schultz T, Dick HB. Small-aperture intraocular lens implantation in a patient with an irregular cornea. J Refract Surg. 2016;32(10):706-708.
4. Hooshmand J, Allen P, Huynh T, et al. Small aperture IC-8 intraocular lens in cataract patients: achieving extended depth of focus through small aperture optics. Eye (Lond). 2019;33(7):1096-1103.
5. Grabner G, Ang RE, Vilupuru S. The small aperture IC-8 intraocular lens, a new concept for added depth of focus in cataract patients. Am J Ophthalmol. 2015;160(6):1176-1184.e1.
