
Surgical refractive correction has come a long way since its inception 30 years ago. Today, we can offer our patients a wide range of lens- and cornea-based refractive surgery procedures, including phakic IOL implantation, refractive lens exchange, LASIK, PRK, and small-incision lenticule extraction (SMILE).
With such a diverse pool of options to choose from, selecting the procedure that is right for each patient can sometimes be a daunting decision; however, in my clinic, we have great faith in the EVO Visian ICL (STAAR Surgical) and continue to expand our recommendations for its use to include low to moderate myopes.
A LONG, SUCCESSFUL HISTORY
Posterior chamber phakic IOLs like the EVO Visian ICL have a 20-year-long history. Clinical validations of safety, efficacy, stability, and predictability for moderate to high myopia and even extremely high myopia are well documented.1,2 Likewise, the phakic IOL can offer many distinct advantages over other refractive surgery procedures. For starters, the Visian ICL has been shown to yield better simulated retinal image quality versus LASIK. In a study of 39 eyes, 20 that received the Visian ICL and 19 that underwent LASIK, mean postoperative coma was 0.17 and 0.37, respectively, and the mean total higher-order aberrations (HOAs) was 0.41 and 0.62, respectively.3 In another study of 93 eyes, 46 that received the Visian ICL and 47 that underwent wavefront-guided LASIK, the ICL induced significantly fewer HOAs than LASIK. Further, in eyes with high myopia, contrast sensitivity improved significantly after implantation of the Visian ICL but deteriorated after wavefront-guided LASIK.4
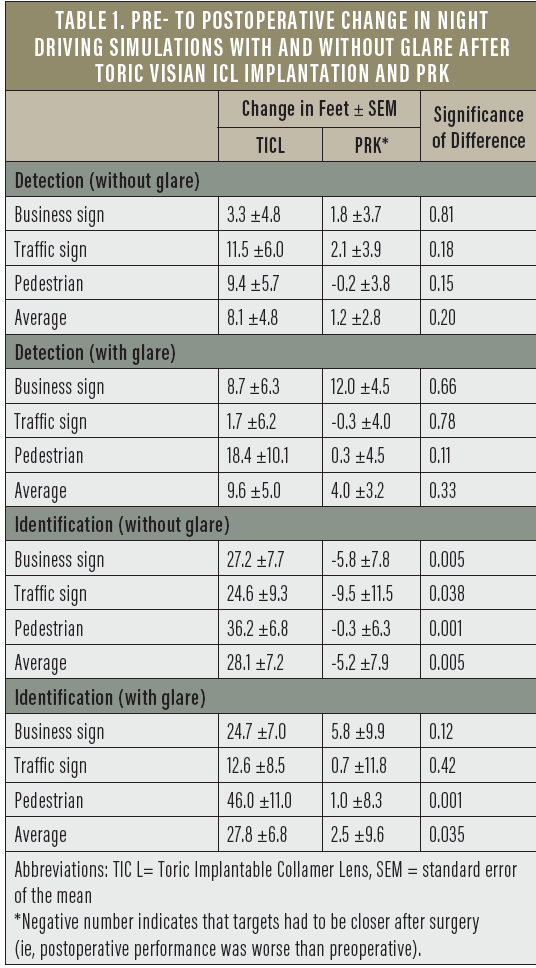
Other studies have also shown that the toric Visian ICL performed better than conventional PRK in pre- to postoperative night driving simulator testing with and without glare.5 In that study of 68 eyes, 27 that received the toric Visian ICL and 41 that underwent PRK, detection and identification of business and traffic signs and pedestrians, both without and with glare, was better in almost every measure. In fact, some patients had to be closer to the object after surgery than they did before surgery to adequately see (Table 1), indicating that the postoperative performance was worse than the preoperative performance in those instances.
EXPANDING PATIENT OPTIONS
Laser vision correction has been shown as an effective means to treat low to moderate myopia, and it is a relatively mature and highly accepted course of treatment. On the other hand, the usefulness of phakic IOLs and SMILE in eyes with low to moderate myopia is not as well documented. In order to assess the EVO Visian ICL and SMILE as alternatives for the correction of low to moderate myopia, my colleagues and I compared and evaluated the clinical outcomes and visual quality after phakic IOL implantation and SMILE for low to moderate myopia.
The sample size of our study included 124 eyes of 63 patients. A total of 75 eyes (38 patients) received the EVO Visian ICL, and 49 eyes (25 patients) underwent SMILE. The average age of patients was similar, at 24.3 ±4.1 years in the ICL group and 25.1 ±5.0 years in the SMILE group. All patients were available for at least 6 months of follow-up. The inclusion criteria were as follows:
- Spherical equivalent (SE) -1.00 to -6.00 D;
- BCVA ≥20/20;
- Anterior chamber depth ≥2.8 mm*;
- Endothelial cell density >2,500 cells/mm2;
- No presence of inflammatory disease;
- No history of trauma; and
- No history of systemic disease.
No intra- or postoperative complications occurred at any point in the study, and all eyes had a normal IOP postoperatively. In the EVO Visian ICL group, the lens vault was stable through 6 months postoperatively.
At 1, 3, and 6 months postoperative, we evaluated UCVA, refractive error, total HOAs, total spherical aberration, and total coma, and we performed a quantitative assessment of visual acuity. By 6 months postoperative, UCVA and BCVA were similar between groups, with average UCVAs in the EVO Visian ICL and SMILE groups of 1.19 ±0.20 and 1.21 ±0.16, respectively, and average BCVAs of 1.22 ±0.11 and 1.23 ±0.13, respectively (Figure 1). Distance UCVA was also similar between groups at 6 months postoperative, with 100% of patients in both the EVO Visian ICL and SMILE groups achieving 20/20 and 71.8% and 73.8%, respectively, achieving 20/16 distance UCVA. More patients in the EVO Visian ICL group achieved 20/12.5, however (24.9% vs 18.8%).
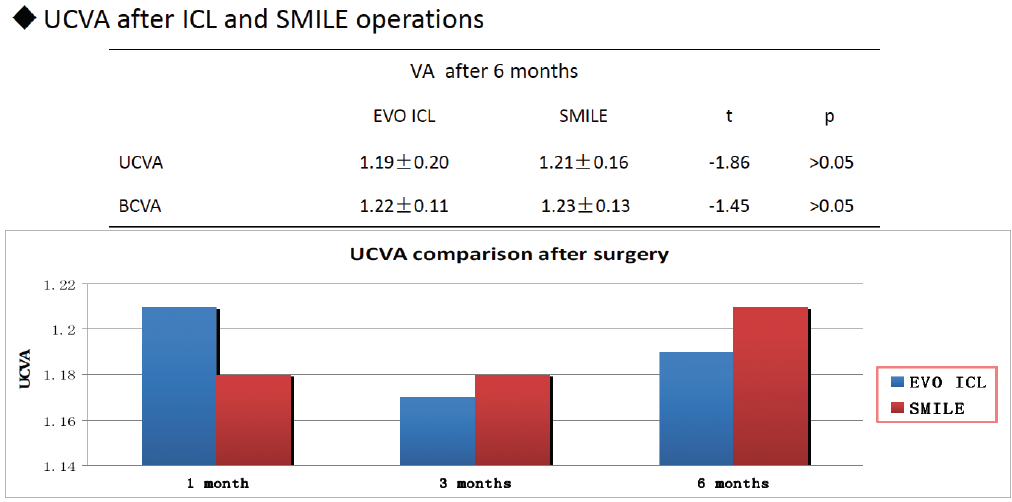
Figure 1. Postoperative UCVA and BCVA: EVO Visian ICL versus SMILE.
When we evaluated postoperative SE, we found that it improved more substantially over time with the EVO Visian ICL. By 6 months postoperative, SE in that group was 0.002 ±0.08, versus -0.085 ±0.18 in the SMILE group (Figure 2). We also found a higher level of refractive predictability in the ±0.50 D range, with 100% of eyes in the EVO Visian ICL group versus 93% in the SMILE group achieving this range.
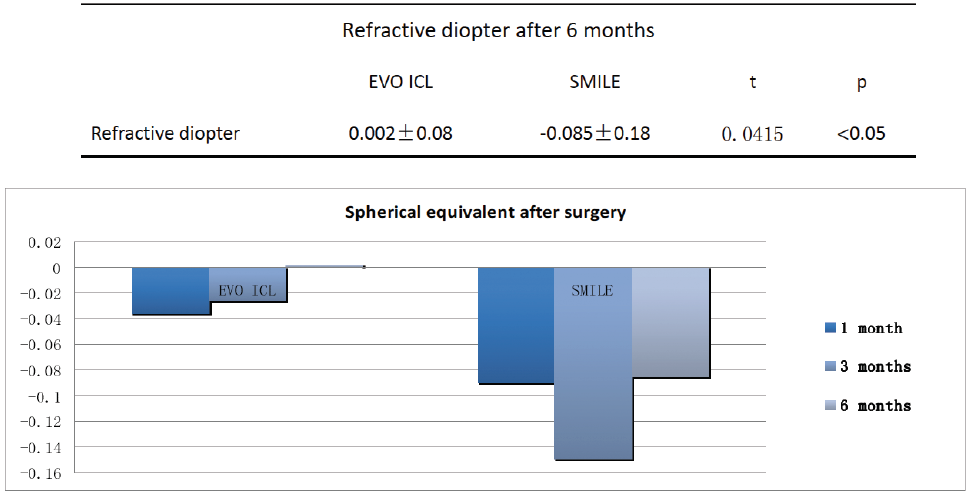
Figure 2. Postoperative spherical equivalent: EVO Visian ICL versus SMILE.
The level at which root mean square HOAs, coma, and sphere increased postoperatively was also slightly higher in the SMILE group (Figure 3), indicating that the quality of vision with the EVO Visian ICL is better than with SMILE. In the quantitative assessment of visual acuity, 26% and 41% of patients in the EVO Visian ICL and SMILE groups, respectively, said that they noticed halos; 10% and 17%, respectively, said that they noticed glare; and 21% and 10%, respectively, said that they noticed starbursts. We used the iTrace (Tracey Technologies), simulated by single HOAs, to determine visual quality and found a corresponding relationship between the amount of spherical aberration (HOAs) and the decreasing visual quality.
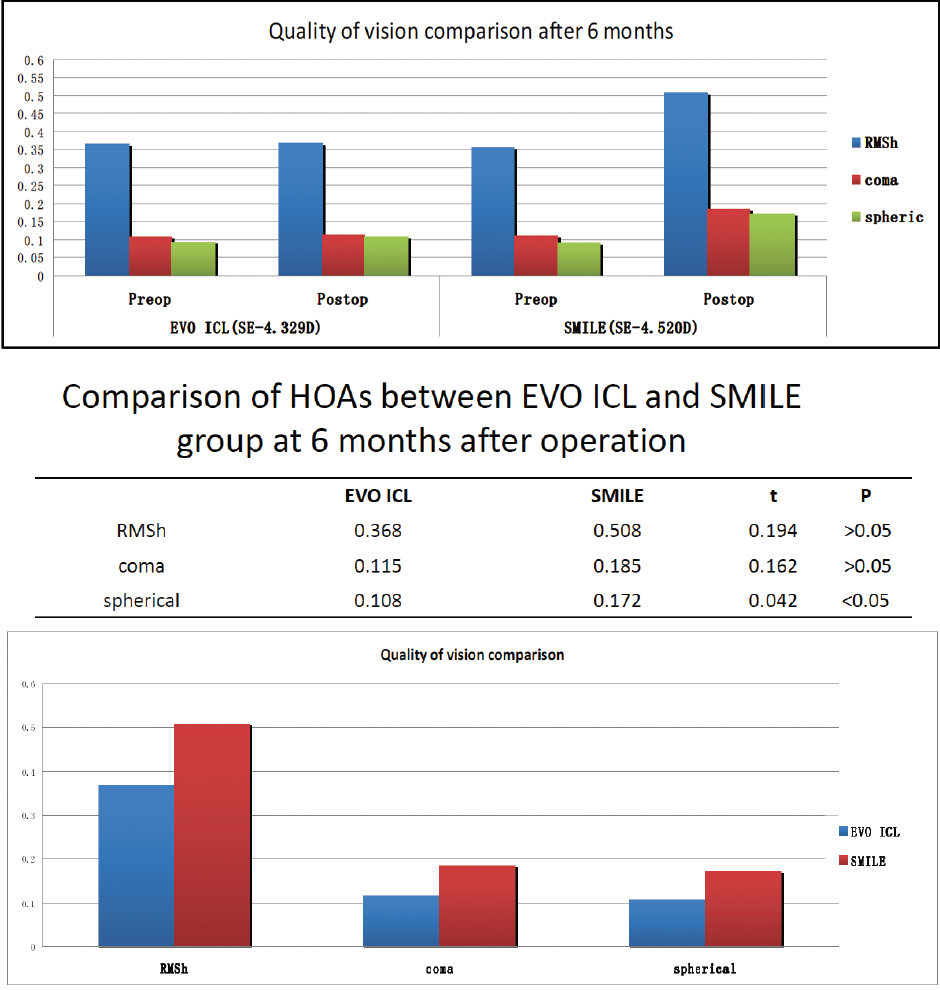
Figure 3. Comparison of quality of vision (top) and HOAs (bottom): EVO Visian ICL versus SMILE.
CONCLUSION
Using our results for grounds to expand the indications for the EVO Visian ICL, we now feel comfortable treating patients with low to moderate myopia with this surgical intervention. In our study, both the EVO Visian ICL and the SMILE procedures provided patients with good clinical outcomes, and both procedures were safe and efficacious. The stability and predictability were better in the EVO Visian ICL group, with 100% of patients achieving a correction within ±0.50 D of the intended refraction. The amount of HOAs was also much lower in the EVO Visian ICL group.
Although both procedures are equivalent in some aspects, I prefer the EVO Visian ICL and believe it is a valid choice for patients with low myopia, especially if the patient has poor preoperative distance BCVA, if the procedure is a second intervention, if the cornea is abnormal, or if the patient has any symptoms of dry eye disease.
1. Igarashi A, Shimizu K. Eight-year follow-up of posterior chamber phakic intraocular lens implantation for high myopia. Am J Ophthalmol. 2014;157(3):532-539.
2. Sanders DR, Doney K, Poco M. ICL in treatment of myopia study group, United States Food and Drug Administration clinical trial of implantable collamer lens (ICL) for moderate to high myopia: Three-year follow-up. Ophthalmol. 2004;111(9):1683-1692.
3. Sarver EJ, Sanders DR, Vukich JA. Image quality in myopic eyes corrected with laser in situ keratomileusis and phakic intraocular lens. J Refract Surg. 2003;19(4):397-404.
4. Igarashi A, Kamiya K, Shimizu K, Komatsu M. Visual performance after implantable collamer lens implantation and wavefront-guided laser in situ keratomileusis for high myopia. Am J Ophthalmol. 2009;148(1):164-170.
5. Schallhorn S, Tanzer D, Sanders DR, et al. Night driving simulation in a randomized prospective comparison of Visian toric implantable collamer lens and conventional PRK for moderate to high myopic astigmatism. J Refract Surg. 2010; 26(5):321-326.

