





Ocular surface disease encompasses a variety of conditions. The limited treatment options for five in particular—persistent epithelial defect (PED), neurotrophic keratopathy (NK), corneal neuralgia, corneal haze, and autoimmune keratoconjunctivitis—frustrate clinicians. A growing understanding of the signalling pathways involved in corneal physiology and healing is allowing the development of new treatments and the repurposing of drugs with established uses in other systemic conditions. This article provides a brief overview of emerging options for treating the big five corneal challenges.
INSULIN FOR PEDS
PEDs are corneal defects that persist for more than 2 weeks despite therapy. Left untreated, PEDs can lead to scarring, infection, and melting.1,2 Conditions impairing the normal healing process of the cornea can cause PEDs by inhibiting reepithelialization.1
Insulin and insulin growth factor receptors, which are necessary for cell proliferation and differentiation, are expressed by corneal epithelial cells.3 Recent studies have shown that both diabetic and nondiabetic patients with serious ocular comorbidities and PEDs can benefit from the administration of topical insulin eye drops when initial treatment fails.1,2 The etiology of the PEDs seems to determine the response to topical insulin; for example, neurotrophic PEDs after vitrectomy tend to respond more favorably than PEDs that are infectious or related to a chemical injury.2 Response is likely mediated by variations in injury severity resulting from different etiologies.
In a study comparing topical insulin to autologous serum, more patients treated with topical insulin experienced reepithelialization, and the mean time to reepithelialization was shorter.2 This was true even among individuals with infectious PEDs that were difficult to treat (Figure 1).There is no consensus on the optimal preparation of topical insulin. Studies often employ artificial tears with polyethylene glycol or propylene glycol as the vehicle and use doses of insulin ranging from 1 to 100 IU/mL.4
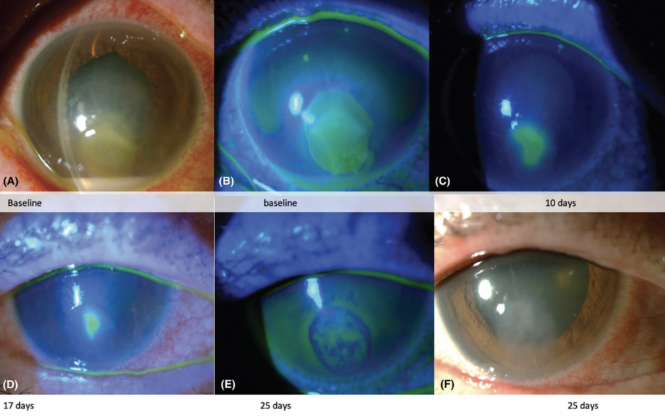
Figure 1. Serial slit-lamp images of the eye of a patient with an infectious PED treated with topical insulin. Reprinted with permission from Diaz-Valle D et al.2
NERVE GROWTH FACTOR FOR NK
Corneal nerves and epithelium share a complex interplay of trophic factors that maintain corneal integrity.5 Corneal nerve degeneration can lead to NK. The condition is characterized by reduced nerve sensation, epithelial breakdown, and an increased risk of infection.5 Disease progression decreases patients’ quality of life and increases their risk of PEDs, stromal melt, perforation, ulceration, and vision loss.6
Treatment with nerve growth factor (NGF) can improve the corneal nerve–epithelium interface by supporting the healing and maintenance of the sensory and sympathetic neurons and the proliferation and migration of epithelial and limbal cells.7,8 Cenegermin-bkbj ophthalmic solution 0.002% (20 µg/mL; Oxervate, Dompé), a recombinant human NGF, is approved by the FDA and European Medicines Agency for the treatment of NK. The drug is administered six times per day for 8 weeks.5,9 In clinical trials, cenegermin increased the rate of corneal healing, and it reduced lesion size, disease progression, and disease recurrence.9 The drug can also enhance nerve regrowth and corneal sensitivity in eyes with NK (Figure 2).9-13
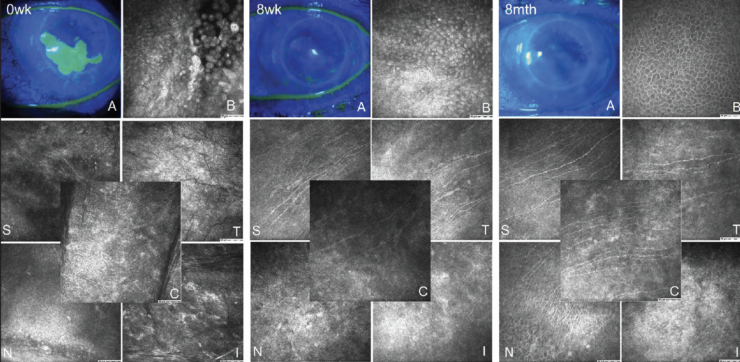
Figure 2. Representative images of a patient with NK treated with cenegermin. The series includes fluorescein staining of the surface of the cornea and in vivo confocal microscopy of the central and peripheral cornea (B, epithelium of the ulcer; C, central; I, inferior; N, nasal; S, superior; T, temporal). At baseline, there was extensive fluorescein staining (A), loose epithelial cells (B), and a few nerves visible superiorly (S). By the end of therapy at 8 weeks, the ulcer has completely closed, as seen on fluorescein staining (A). There is continued epithelial growth (B) and increased nerve growth superiorly (S) and temporally (T) with few immature nerves centrally (C). At the 8-month follow-up visit, there is no longer any appreciable fluorescein staining (A), the ulcer has healed with mature epithelium (B), and subbasal corneal nerves are present throughout the superior (S), temporal (T), central (C), and nasal (N) sectors. This image by Pedrotti et al is used under CC BY 4.0 Deed.13
Another topical agent, pergolide, increases NGF expression through dopamine receptor agonism and has demonstrated efficacy in corneal nerve regeneration and wound healing in mice.14
NALTREXONE FOR CORNEAL NEURALGIA
Damage to the sensory nerves of the cornea can lead to persistent feelings of pain and irritation.15 The causes of corneal neuralgia include trauma, chemical injury, ocular surface disease, and anterior segment surgery. The condition frustrates patients and doctors alike because the pain is significant and persistent in the absence of corneal findings at the slit lamp.
Corneal neuralgia is challenging to treat owing to central sensitization.15 Low-dose naltrexone (LDN) has demonstrated success for the treatment of neuropathic pain caused by other diseases. Researchers are therefore investigating the drug’s use in corneal neuralgia.16 The therapeutic effect of LDN manages both central and peripheral components of pain. The drug works through a transient blockade of μ and delta opioid receptors to increase the release of endogenous endorphins. LDN also has an antiinflammatory effect as a toll-like receptor 4 antagonist.17,18
A novel study investigated the use of LDN in patients with corneal neuralgia.16 A dose of 4.5 mg/day (escalated from an initial dose of 1.5 mg/day) of oral LDN successfully treated corneal neuralgia during the 4-week study period. LDN was well tolerated; patients reported a significant improvement in pain, discomfort, and quality of life.
Naltrexone can also be prepared as a topical ophthalmic formulation 0.4 mg/mL.
LOSARTAN FOR CORNEAL HAZE
Disordered healing after insult may lead to corneal opacification. Transforming growth factor (TGF) beta from the epithelium is activated in response to injury. This multifunctional cytokine migrates from the epithelium, aqueous humor, tears, and endothelial cells to the stroma and subsequently activates myofibroblasts.19-21 TGF beta expression typically decreases over time. If expression is prolonged, myofibroblasts continue to produce disordered extracellular matrix that opacifies the cornea.19
Losartan is an angiotensin 2 receptor blocker used to treat hypertension. The drug also attenuates TGF beta signaling and has successfully passed through intact epithelium to the corneal stroma in rabbits.22 Treatment can cause apoptosis of myofibroblasts that rely on TGF beta signaling for survival, allow fibroblasts to regenerate the basement membrane, and decrease haze.19,22 Losartan is therefore well suited for the management of persistent corneal haze from a variety of conditions.19 In contrast, other topical drugs used to treat corneal haze, such as corticosteroids and mitomycin C, have limited efficacy once fibrosis develops, and they are associated with significant adverse effects with long-term use.22
After years of encouraging results in animal studies, the first human case report of the successful use of topical losartan (0.8 mg/mL in sodium chloride 0.9%) for corneal haze after a refractive procedure was published in 2022.20 The patient was initially treated with one drop administered six times per day for 1 month. Dosing was subsequently reduced to one drop administered four times per day for another 4 months. During this period, corneal haze decreased significantly. In addition, the patient’s uncorrected distance visual acuity improved from 20/80 to 20/30, and their corrected distance visual acuity improved from 20/25 with a refraction of -1.25 -1.00 x 175º to 20/25 with a refraction of -0.50 -1.25 x 3º.
TACROLIMUS FOR AUTOIMMUNE KERATOCONJUNCTIVITIS
Corticosteroids are used to treat a variety of inflammatory ocular diseases. The strategy is efficacious but suboptimal for many autoimmune conditions because a prolonged course of steroids may lead to cataract formation, infection, and glaucoma.
Tacrolimus, a macrolide that is one to 100 times more potent than cyclosporine, works by inhibiting calcineurin in T lymphocytes to decrease inflammatory cell activity and the release of inflammatory cytokines.23,24 Autoimmune disorders such as vernal keratoconjunctivitis, ocular graft-versus-host disease, autoimmune polyglandular syndrome-1 keratitis, dry eye due to Sjögren syndrome, chronic anterior uveitis, Stevens-Johnson syndrome, and ocular cicatricial pemphigoid have been successfully treated with tacrolimus.23 The drug has a high molecular weight. Its lipophilicity makes tacrolimus more successful at penetrating the conjunctiva than the cornea, so the drug is particularly effective at treating the conjunctival component of inflammatory disorders.23
Although tacrolimus is generally well tolerated, it is associated with side effects such as irritation and an increased risk of infection.23 Patients with concomitant atopic dermatitis should be closely monitored owing to reports of an increased risk of herpes simplex infection and T-cell lymphoma.
The concentration and dosing frequency of tacrolimus vary among studies and conditions treated (0.02%–0.1% and 1–4 times per day).23 Tacrolimus is commercially available as a 0.03% or 0.1% ointment (Protopic, Astellas Pharma US), which may be used off-label one to four times per day. Alternatively, the drug may be administered orally once per day in doses ranging from 0.5 to 5 mg.
CONCLUSION
Many patients are affected by the big five corneal challenges. The severe pain and discomfort they cause reduce patients’ quality of life. Promising results to date suggest that the drugs discussed in this article can enhance patient care and mitigate the use of treatments that may be more invasive or associated with greater side effects. Further studies to establish the safety and efficacy of these novel agents are warranted.
1. Diaz-Valle D, Burgos-Blasco B, Gegundez-Fernandez JA, et al. Topical insulin for refractory persistent corneal epithelial defects. Eur J Ophthalmol. 2021;31(5):2280-2286.
2. Diaz-Valle D, Burgos-Blasco B, Rego-Lorca D, et al. Comparison of the efficacy of topical insulin with autologous serum eye drops in persistent epithelial defects of the cornea. Acta Ophthalmol. 2022;100(4):e912-e919.
3. Yu FS, Yin J, Xu K, Huang J. Growth factors and corneal epithelial wound healing. Brain Res Bull. 2010;81(2-3):229-235.
4. Castro Mora MP, Palacio Varona J, Perez Riaño B, Laverde Cubides C, Rey-Rodriguez DV. Effectiveness of topical insulin for the treatment of surface corneal pathologies. Arch Soc Esp Oftalmol (Engl ed). 2023;98(4):220-232.
5. NaPier E, Camacho M, McDevitt TF, Sweeney AR. Neurotrophic keratopathy: current challenges and future prospects. Ann Med. 2022;54(1):666-673.
6. Saad S, Abdelmassih Y, Saad R, et al. Neurotrophic keratitis: frequency, etiologies, clinical management and outcomes. Ocul Surf. 2020;18(2):231-236.
7. Blanco-Mezquita T, Martinez-Garcia C, Proença R, et al. Nerve growth factor promotes corneal epithelial migration by enhancing expression of matrix metalloprotease-9. Invest Ophthalmol Vis Sci. 2013;54(6):3880-3890.
8. Lambiase A, Bonini S, Aloe L, Rama P, Bonini S. Anti-inflammatory and healing properties of nerve growth factor in immune corneal ulcers with stromal melting. Arch Ophthalmol. 2000;118(10):1446-1449.
9. Pflugfelder SC, Massaro-Giordano M, Perez VL, et al. Topical recombinant human nerve growth factor (cenegermin) for neurotrophic keratopathy: a multicenter randomized vehicle-controlled pivotal trial. Ophthalmology. 2020;127(1):14-26.
10. Meduri A, Oliverio GW, Valastro A, et al. Neurotrophic keratopathy in systemic diseases: a case series on patients treated with rh-NGF. Front Med (Lausanne). 2022;9:920688.
11. Roszkowska AM, Inferrera L, Aragona E, Gargano R, Postorino EI, Aragona P. Clinical and instrumental assessment of the corneal healing in moderate and severe neurotrophic keratopathy treated with rh-NGF (cenegermin). Eur J Ophthalmol. 2022;32(6):3402-3410.
12. Mastropasqua L, Lanzini M, Dua HS, et al. In vivo evaluation of corneal nerves and epithelial healing after treatment with recombinant nerve growth factor for neurotrophic keratopathy. Am J Ophthalmol. 2020;217:278-286.
13. Pedrotti E, Bonacci E, Chierego C, et al. Eight months follow-up of corneal nerves and sensitivity after treatment with cenegermin for neurotrophic keratopathy. Orphanet J Rare Dis. 2022;17(1):63.
14. Zhang X, Muddana S, Kumar SR, et al. Topical pergolide enhance corneal nerve regrowth following induced corneal abrasion. Invest Ophthalmol Vis Sci. 2020;61(1):4.
15. Goyal S, Hamrah P. Understanding neuropathic corneal pain—gaps and current therapeutic approaches. Semin Ophthalmol. 2016;31(1-2):59-70.
16. Dieckmann G, Ozmen MC, Cox SM, Engert RC, Hamrah P. Low-dose naltrexone is effective and well-tolerated for modulating symptoms in patients with neuropathic corneal pain. Ocul Surf. 2021;20:33-38.
17. Younger J, Parkitny L, McLain D. The use of low-dose naltrexone (LDN) as a novel anti-inflammatory treatment for chronic pain. Clin Rheumatol. 2014;33(4):451-459.
18. Toljan K, Vrooman B. Low-dose naltrexone (LDN)-review of therapeutic utilization. Med Sci (Basel). 2018;6(4):82.
19. Wilson SE. Topical losartan: practical guidance for clinical trials in the prevention and treatment of corneal scarring fibrosis and other eye diseases and disorders. J Ocul Pharmacol Ther. 2023;39(3):191-206.
20. Pereira-Souza AL, Ambrósio R Jr, Bandeira F, Salomão MQ, Souza Lima A, Wilson SE. Topical losartan for treating corneal fibrosis (haze): first clinical experience. J Refract Surg. 2022;38(11):741-746.
21. Singh V, Jaini R, Torricelli AA, et al. TGFß and PDGF-B signaling blockade inhibits myofibroblast development from both bone marrow-derived and keratocyte-derived precursor cells in vivo. Exp Eye Res. 2014;121:35-40.
22. Sampaio LP, Hilgert GSL, Shiju TM, Murillo SE, Santhiago MR, Wilson SE. Topical losartan inhibits corneal scarring fibrosis and collagen type IV deposition after Descemet’s membrane-endothelial excision in rabbits. Exp Eye Res. 2022;216:108940.
23. Shoughy SS. Topical tacrolimus in anterior segment inflammatory disorders. Eye Vis (Lond). 2017;4:7.
24. Sawada S, Suzuki G, Kawase Y, Takaku F. Novel immunosuppressive agent, FK506. In vitro effects on the cloned T cell activation. J Immunol. 1987;139(6):1797-1803.
