



LASIK and PRK were primary refractive procedures 15 to 20 years ago. Recent advances in phakic and premium IOLs have encouraged more ophthalmologists to engage in refractive surgery, including refractive lens exchange, with a greater overall emphasis on correcting presbyopia and astigmatism. This evolution is supported by a concurrent shift in patients’ attitudes. Thanks to the large volume of refractive procedures performed during the past 25 years, many potential patients now have friends and/or family members who have undergone surgery that reduced or eliminated their dependence on spectacles and contact lenses. Consequently, public interest in refractive surgery, including refractive cataract surgery, has grown.
To further expand the field of refractive surgery, it is crucial to widen the pool of potential candidates. Technological advances play a pivotal role in this endeavor.
LENS-BASED REFRACTIVE SURGERY
Myopia. A significant driver of the growth of refractive surgery in my practice has been the introduction of the EVO ICL (STAAR Surgical). This advancement over the original ICL has improved the patient experience—eliminating the need for laser peripheral iridotomies—and safety. The EVO ICL has also broadened the pool of candidates for this technology. Earlier ICLs were reserved for patients with extremely high refractive errors, but individuals with as little as 3.00 D of myopia can be excellent candidates for the EVO ICL. My patients also appreciate that the procedure is reversible.
A particularly promising group for the EVO ICL is keratoconic patients with high myopia. Although implanting the lens does not negate the need for scleral lenses in patients with irregular astigmatism, it does help improve overall vision by correcting high myopia (Figure 1).
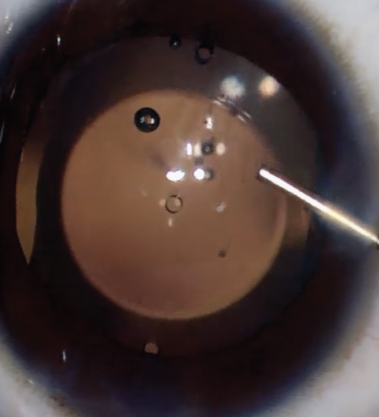
Figure 1. Intraoperative image of an EVO ICL in situ.
Presbyopia. Expanded and improved IOL options have spurred an increase in the number of ophthalmologists offering surgery to address presbyopia. In our surgery center, for example, the percentage of surgeons placing presbyopia-correcting IOLs has increased from 80% (12 of 15) to 94% (15 of 16) in the past 3 years. The availability of multifocal, bifocal, extended depth of focus, small-aperture, and monofocal plus IOLs has led to an increase in the number of ophthalmologists offering surgery for presbyopia. This variety allows for customized approaches in cataract surgery and refractive lens exchange to meet individual patient needs.
Irregular corneas. Patients with irregular corneas, such as those resulting from previous corneal refractive surgery (including radial keratotomy), may greatly benefit from the Light Adjustable Lens (RxSight). The complexity of IOL power calculations in this population is well known, and refractive surprises are common. The LAL permits the postoperative refinement of refractive outcomes (Figure 2), making multifocal correction a viable option. I have also found the LAL effective for patients accustomed to monovision contact lens wear who wish to replicate this strategy. Furthermore, RxSight recently introduced a new LAL model offering extended depth of focus, expanding the options available for patients.
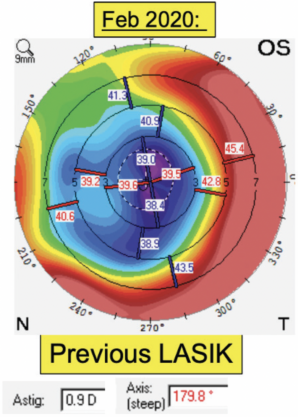
Figure 2. A 69-year-old patient underwent cataract surgery with LAL implantation. Following surgery, their UCVA was 20/40. After light adjustments were performed, their final UCVA was 20/25.
THE NEXT HURDLE
An unmet need is a reliable surgical method for maintaining accommodation as people age. One technology currently in development is a laser treatment targeting the sclera to reduce its rigidity (Ace Vision). Another innovative approach involves implanting microinserts in the sclera (Refocus Group). The goal of both approaches is to restore accommodation.
CONCLUSION
Recent technological advances are expanding the options for refractive surgery. They are not only broadening the pool of candidates and improving surgical outcomes but also fostering a refractive mindset among both patients and providers. Patient selection remains key to success with these procedures. Surgeons must be able to determine which procedure is likely to deliver the most satisfactory outcome to each patient.
