


Patients who are emmetropic after LASIK are typically the most bothered by the onset of presbyopia and the most willing to do something about it. They are sensitive to changes in their vision and, unlike their myopic counterparts, cannot remove their glasses to read or cheat presbyopia with contact lens mini-monovision. The sudden need for reading glasses sends many of these patients back to their refractive surgeon because they worry that something is terribly wrong or think that the LASIK procedure has, as many patients put it, “worn off.”
I have been unenthusiastic about the limited and suboptimal opportunities for presbyopia correction that I can offer to these patients. LASIK is not an option for them, and therefore a monovision enhancement performed many years after LASIK would have to be PRK. The results of this procedure are less predictable when it is performed after LASIK,1,2 and it carries the risk of haze.
Refractive lens exchange is not an optimal alternative for emmetropic post-LASIK patients who are in their 40s and early 50s. Those with early presbyopia would lose what accommodative ability they retain, and intraocular surgery is not without risk in this population. Moreover, post-LASIK patients with a history of high myopia may not be good candidates for refractive lens exchange because they are at increased risk of retinal detachment.3
Based on all of these considerations, I generally dissuade post-LASIK patients from undergoing intraocular surgery to address presbyopia until the condition progresses or they develop cataracts. In these situations, the benefits of intervention should begin to outweigh its risks. Many patients are disappointed; they do not want to wear reading glasses after having enjoyed spectacle independence for years before the onset of presbyopia. In the not-too-distant future, pharmacologic solutions to presbyopia may become a good alternative for these and other patients.
TWO MECHANISMS OF ACTION
Presbyopia-correcting drops may be divided into two categories.
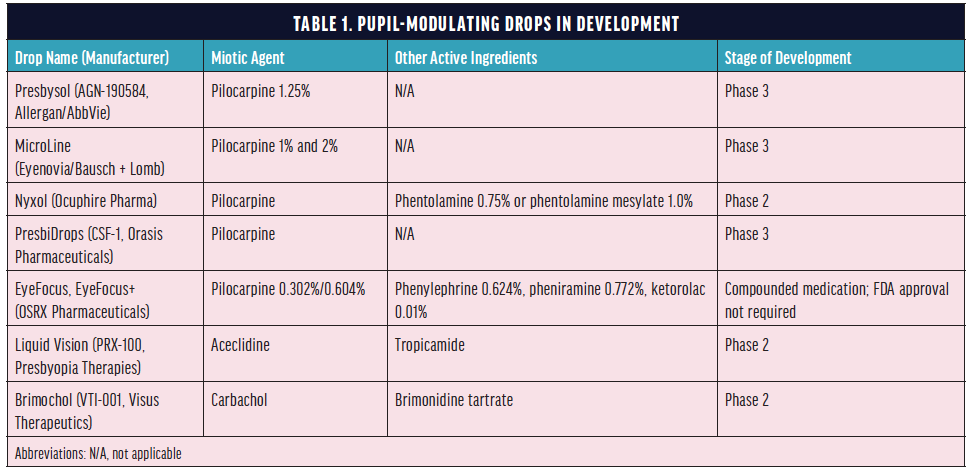
Pupil-modulating drops. Most of the topical agents being developed for the treatment of presbyopia modulate the pupil to increase depth of field through the pinhole effect (Table 1). These drops are instilled daily or as needed to improve near vision. Allergan, Eyenovia/Bausch + Lomb, Ocuphire Pharma, Orasis Pharmaceuticals, OSRX Pharmaceuticals, Presbyopia Therapies, and Visus Therapeutics have products in the pipeline, and some are likely to be available relatively soon.
Lens-restoring drops. This category of presbyopia-correcting drops helps to restore accommodation by softening or altering the crystalline lens (Table 2). Companies developing these drops include Viewpoint Therapeutics and Novartis. Lens-restoring drops will likely be administered for a period of several weeks or months, perhaps every year. The agents must penetrate the cornea and alter the lens anatomy, and long-term studies are therefore required to establish their safety.

POTENTIAL CANDIDATES
I anticipate that pupil-modulating drops will have wide appeal, but my expectation is that emmetropic patients—especially those with a history of LASIK—will be among the earliest adopters. In my practice, the ideal candidates will be 40 to 60 years of age and will not yet have significant lens opacity.
Pupil-modulating drops may also be helpful for addressing higher-order aberrations (HOAs) in post-LASIK eyes. Patients who underwent the procedure before the advent of wavefront-guided technology and blended optical zones often have higher levels of corneal HOAs. For these patients, pupillary miosis is an effective treatment because a small pupillary aperture minimizes the impact of corneal HOAs on vision.4
It is not yet clear which patients will be the best candidates for lens-restoring drops, but I expect such drops may be targeted toward younger presbyopes.
Topical pupil-modulating drops for the treatment of presbyopia are likely to carry minimal risks and should face low barriers to market entry. Similar to multifocal contact lenses and progressive spectacles, patients will be able to try out drops in different settings and over time to determine whether they like them. Unlike surgery, treatment can be reversed simply by ceasing to administer the drops.
PATIENT SELECTION
As clinical trials progress and presbyopia-correcting drops become available, optometrists and ophthalmologists will have to become familiar with the characteristics of these products for the purposes of patient selection and education.
Duration of action. The duration of action—likely to vary among products—is an important consideration, especially for pupil-modulating drops. A patient who works a full-time job will probably desire at least 8 hours of effect in order to see well at near and intermediate distance throughout their shift. On the other hand, a patient who simply wants to avoid wearing reading glasses during weekend dinners with friends may be satisfied with a shorter duration of action. Patient compliance with these drops will likely be high because patients will notice the effects of noncompliance.
Side effects. Miotic agents such as pilocarpine and carbochol have a long history of ophthalmic use and well-established safety profiles. Ongoing clinical trial results will provide data on side effects such as headache, brow ache, constricted field, and difficulty in low-light environments as well as on safety concerns. Some of the presbyopia-correcting drops in development include additional ingredients such as NSAIDs and alpha-2 agonists to modulate the miotic effects and advanced vehicles to increase ocular comfort.
The Potential of Presbyopia Drops
Surgeons share their thoughts on the future use of these medications.
By Jorge L. Alió, MD, PhD, FEBOphth; Jay S. Pepose, MD, PhD; and Sheri Rowen, MD, FACS
An Essential Therapeutic Role
Jorge L. Alió, MD, PhD, FEBOphth

In my opinion, pharmacological strategies for presbyopia correction will play an essential therapeutic role in the treatment of early and intermediate presbyopia. The investigations I have participated in indicate that the pharmacological treatment of presbyopia could also supplement the visual performance of cases in which IOLs are partially insufficient for near vision, such as some accommodating IOLs.
I have been involved in several clinical studies on the pharmacological treatment of presbyopia.1-4 From my experience, I can clearly state that patients are eager for a solution such as this. Patients with early signs of presbyopia are not interested in surgery, and they are not happy to use near vision glasses. Patients with intermediate signs of presbyopia who use glasses for near vision are more motivated to undergo surgery, but most are now more interested in pharmacological solutions. Based on clinical experience, patients with advanced presbyopia do not benefit conveniently from this type of therapy because it is not effective in achieving a satisfactory outcome in full presbyopia.
I am optimistic about the future of pharmacological agents for presbyopia correction. I think they represent an alternative to glasses for patients with signs of early and intermediate presbyopia, and I believe there is an ample market opportunity for the companies entering into this space.
1. Vargas V, Vejarano F, Alio J. Pharmacological therapy for presbyopia in patients with previous corneal refractive surgery: a pilot study. Ophthalmol Ther. 2020;9(4):1003-1010.
2. Vargas V, Vejarano F, Alió JL. Near vision improvement with the use of a new topical compound for presbyopia correction: a prospective, consecutive interventional non-comparative clinical study. Ophthalmol Ther. 2019;8(1):31-39.
3. Renna A, Alió JL, Vejarano LF. Pharmacological treatments of presbyopia: a review of modern perspectives. Eye Vis (Lond). 2017;4:3.
4. Renna A, Vejarano LF, De la Cruz E, Alió JL. Pharmacological treatment of presbyopia by novel binocularly instilled eye drops: a pilot study. Ophthalmol Ther. 2016;5(1):63-73.
A Welcome Offering
Jay S. Pepose, MD, PhD

Presbyopia drops will be a welcome offering for emmetropic presbyopes not suited to or uninterested in refractive lens exchange and for those not tolerant of monovision laser vision correction. Drugs under development are differentiated by their effects on pupil modulation; duration; speed of onset; cost; mechanism of action on the iris sphincter, dilator, or both; ease of application (drops vs directional mist vs transdermal); comfort; tolerability; impact on distance acuity (including under low lighting conditions); and side effects. Factors that may influence drug performance may include late versus early presbyopia with some residual accommodative function, dark versus light irides, habitual pupil size, age, systemic comorbidities such as diabetes, dry eye disease, concurrent systemic and topical medications, manifest refraction, and phakic or pseudophakic status.
Clinical trials are conducted through best distance correction. Patients in real-world settings, however, are not all going to be plano presbyopes. Based on my experience with small-aperture inlays and IOLs, patients slightly on the myopic side may have more enhanced depth of focus with miotics than low hyperopes. Miotics may also improve the efficacy and tolerability of mini-monovision as opposed to full monovision.
Reading performance is highly affected by target luminance.1 Effective pupil modulation may therefore be a delicate balance for each patient because the gain from substantial pupil shrinkage at near defocus declines at low light levels whereas the cost to distance image quality increases by elevating luminance-dependent neural contrast thresholds, which will be compounded in eyes with scatter (eg, dry eye or early nuclear sclerosis). Appropriate dosing of a single formulation drop or spray may become nuanced, and non–fixed-dose drops that separately affect the iris dilator and sphincter may also facilitate titration to optimize pupil size during the course of day. Patients with small pupils at baseline may not experience as great an impact from presbyopia-treating drops.
1. Xu R, Gil D, Dibas M, Hare W, Bradley A. The effect of light level and small pupils on presbyopic reading performance. Invest Ophthalmol Vis Sci. 2016;57(13):5656-5664.
An Unprecedented Disruptor
Sheri Rowen, MD, FACS

We have a busy cataract and refractive practice, and new patients often come in to find out about correcting their loss of near vision. Many of them have seen well at all ranges of distance, and the change to their vision is a disturbing event for these 45-to-55-year-old individuals with plano presbyopia, often representing the first sign of aging. Even those who have worn contact lenses for distance correction experience near vision loss and wear glasses over their contact lenses.
If presbyopia drops become a part of everyday practice, I will start using this treatment in plano presbyopes and mild hyperopes to try to delay their need for glasses. For anyone who has a significant need for contacts, I will try laser vision correction first and add the drops thereafter if needed. Topical drops would be a great entrée into our ophthalmology and optometry practices, allowing us to develop patients presenting for presbyopia treatment into long-term patients while assuring them that we are suggesting the correct modes of treatment as we all age together. I would always try to optimize patients’ distance vision, even in monofocal glasses, contacts, or mini-monovision in hopes they do not instantly need bifocals.
A topical drop for presbyopia would be ideal if it worked, did not cause side effects, and was comfortable upon administration. Patients with presbyopia are looking for an alternative to readers. If they can simply administer drops a few times a day as needed instead of wearing readers, the presbyopia market could be disrupted in a way we never imagined.
PATIENT EDUCATION
The development of presbyopia-correcting drops is already changing my conversations with post-LASIK patients. For now, I recommend that those with early presbyopia who are seeking an enhancement use low-powered readers until these drops become available. Knowing that this therapy is on the horizon also makes me more comfortable offering LASIK to patients who are in their late 30s and will soon become presbyopic.
As this category evolves, practitioners will have to determine how best to counsel patients. Just as lifestyle questionnaires are used to ascertain patient needs and expectations for presbyopia-correcting IOLs, questionnaires may have to be developed to help customize pharmacologic presbyopia therapy to patients’ lifestyles and even their needs on a particular day. A period of adjustment may be required to determine the ideal time(s) of day to instill pupil-modulating drops. I am confident, however, that post-LASIK patients will persevere in order to enjoy the benefits of a noninvasive form of correction.
CONCLUSION
Presbyopia-correcting eye drops will be an exciting option for patients who are not yet ready for intraocular surgery, whether or not they have a history of LASIK. I expect these agents to become available in the next few years.
1. Moshirfar M, Jehangir N, Fenzl CR, McCaughey M. LASIK enhancement: clinical and surgical management. J Refract Surg. 2017;33(2):116-127.
2. Lee BS, Gupta PK, Davis EA, Hardten DR. Outcomes of photorefractive keratectomy enhancement after LASIK. J Refract Surg. 2014;30(8):549-556.
3. Ullrich M, Zwickl H, Findl O. Incidence of rhegmatogenous retinal detachment in myopic phakic eyes. J Cataract Refract Surg. September 7, 2020. doi:10.1097/j.jcrs.0000000000000420
4. Dick HB. Small-aperture strategies for the correction of presbyopia. Curr Opin Ophthalmol. 2019;30(4):236-242.
5. Stamper R, Lieberman M, Drake M. Becker-Shaffer’s Diagnosis and Therapy of the Glaucomas. 8th ed. Mosby; 2009.
