



Oculoplastic surgery has become an important tool for ophthalmologists, particularly because patient interest in eyelid surgery has grown. The COVID-19 pandemic has contributed to this growth. When wearing a face mask, people’s expressions are limited mainly to their eyes and eyelids. At my practice, the demand for eyelid surgery increased by 15% over the past 2 years. Comprehensive ophthalmologists who wish to begin offering oculoplastic surgery may therefore wish to focus first on the eyelids.
THE EVALUATION
The general aim of patients considering an eyelid procedure is to look like themselves—only better. As with other forms of elective surgery, it is important for surgeons and staff to help patients establish realistic expectations. A thorough preoperative examination is essential to maximizing safety and optimizing outcomes. Photographs are taken of the eyelids, face, and sideview and compared to photographs that depict how the patient looked at a younger age.
When planning surgery, it is important to respect the fullness of the patient’s eyelids. The fat pads are evaluated, and a pinch test is performed to detect laxity in the lower eyelid. If the patient has received injections of botulinum toxin in their forehead, this must be considered when determining the amount of skin to be excised.
SURGERY
Many of my patients who wish to improve the appearance of their eyelids elect to receive a combination of three procedures—a neuromodulator, a dermal filler, and blepharoplasty.
I began using a CO2 laser (Lumenis, MediVision) more than a decade ago for both upper and lower eyelid blepharoplasty. Compared to surgery with a scalpel, patient satisfaction is high with this technology because laser blepharoplasty is a bloodless, quicker procedure and it causes less bruising. In my experience, the CO2 laser also enhances precision. Patients, moreover, generally find laser surgery more appealing. The concept of undergoing manual surgery with a scalpel may frighten them off.
Upper eyelid blepharoplasty. This popular procedure can include skin excision, vaporization of the medial fat pad, and sculpting of retro–orbicularis orbital fat.
Male and female eyelids differ in appearance (Figures 1 and 2), so the surgical approach must be tailored to each patient. For a feminine appearance, target an upper lid crease at a height of 4 mm. The incision is created 8 mm above the eyelashes and at least 10 mm away from the lower part of the eyebrow (Figure 3). For a more masculine appearance, excise less skin.
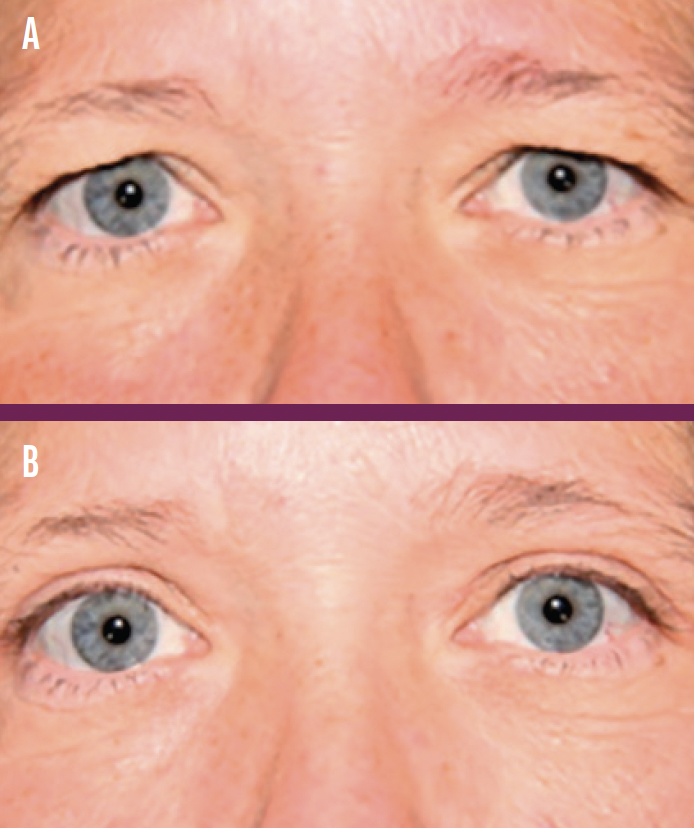
Figure 1. Before (A) and after (B) photographs taken of a man who underwent upper eyelid blepharoplasty.
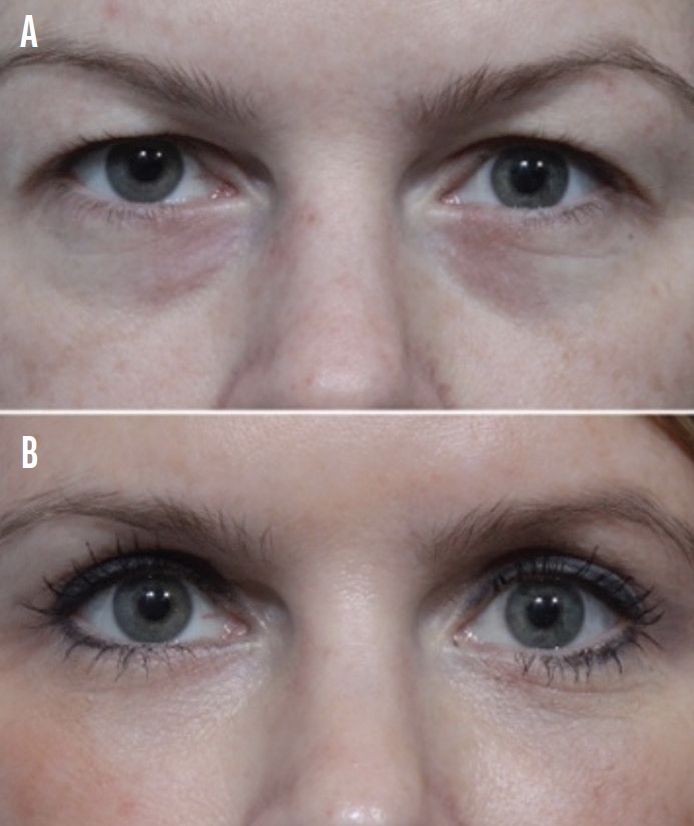
Figure 2. Before (A) and after (B) photographs taken of a woman who underwent upper eyelid blepharoplasty.
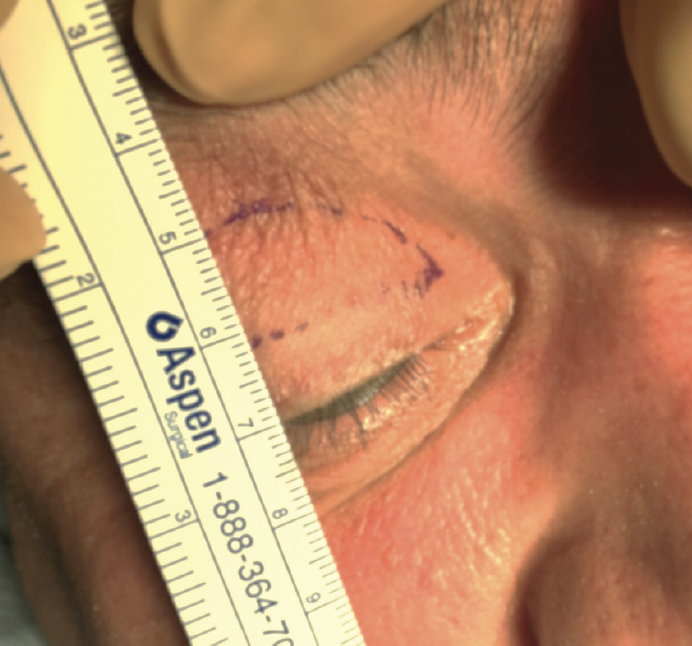
Figure 3. Preoperative planning for an upper eyelid blepharoplasty.
Lower eyelid blepharoplasty. Surgery on the lower eyelid is more complex than upper eyelid blepharoplasty because of possible lid laxity that must be addressed. Many older patients with baggy eyelids present with epiphora. Ideally, a lower eyelid has a downward vector that promotes tear flow. The tears follow the gravity from the lateral to medial lower part of the eyelid. A patient with baggy eyelids therefore often presents with epiphora.
Various surgical approaches to lower eyelid blepharoplasty are used (Figure 4). One of these is a transconjunctival internal approach toward an external incision combined with a lateral canthoplasty. Depending on the degree of eyelid laxity, the lateral tarsus may be tucked into the lateral orbital rim, or a lateral tarsal strip procedure may be performed (Figure 5). Additional approaches include the creation of a musculocutaneous flap and a fat-redraping technique. In the latter, fat is redraped over the orbital rim to solve a marked tear trough. Skin resection must be limited to a maximum of 5 mm.
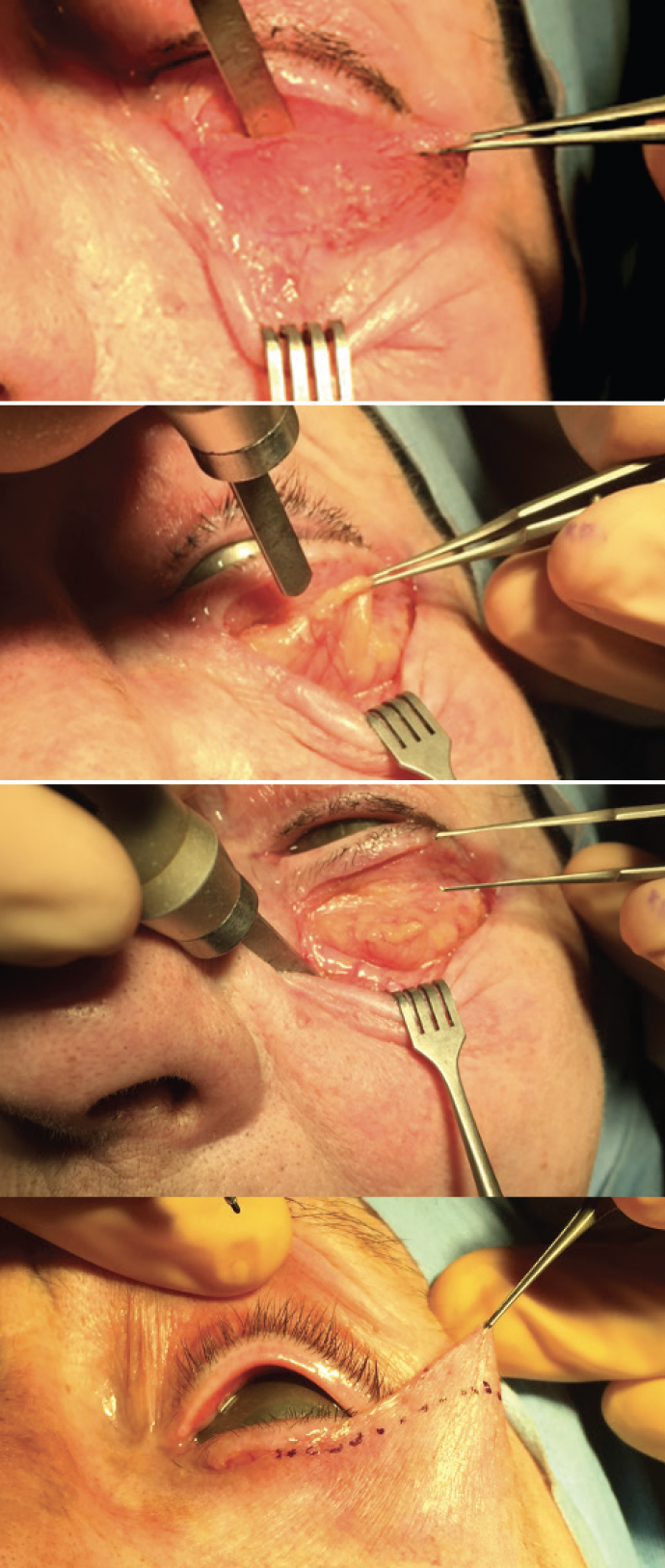
Figure 4. Lower eyelid blepharoplasty.

Figure 5. A lateral tarsal strip procedure.
A careful preoperative examination can facilitate the choice of surgical approach.
Combining surgery on the upper and lower eyelids. A transconjunctival approach in lower eyelid blepharoplasty may be combined with upper eyelid blepharoplasty in a single session. If the preoperative examination demonstrates eyelid laxity, however, an external approach to lower lid blepharoplasty is required, and the lateral canthus must be addressed (Figure 6). In these situations, I prefer to do the surgery in two steps because of the risk of lymphedema when both upper and lower eyelids are treated in one session.
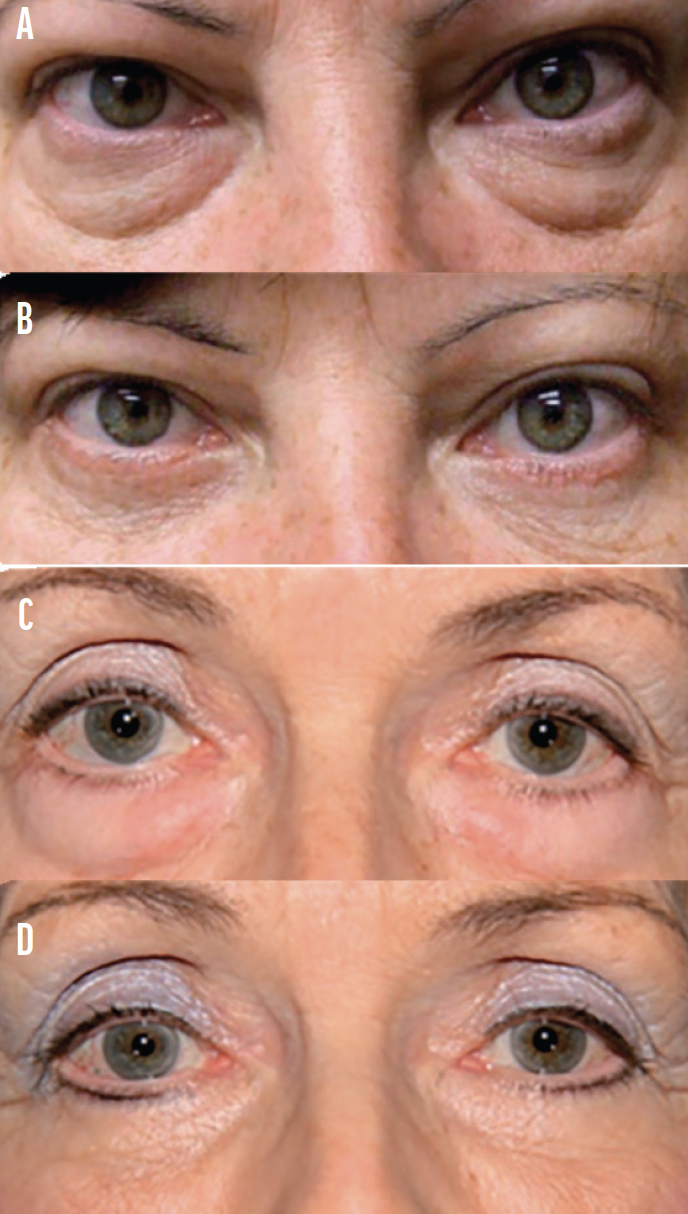
Figure 6. Examples of before (A, C) and after (B, D) photographs taken of two patients who underwent a lower eyelid blepharoplasty procedure with an external approach.
COMPLICATIONS
When rules such as those described in this article are respected, complications from blepharoplasty are rare and typically can be resolved. The most serious potential complication is a retrobulbar hemorrhage in the retroseptal intraorbital region. The response must be rapid to coagulate the bleeding vessel. Additional complications can include wound dehiscence (Figure 7), postoperative asymmetry of the upper lid crease, and a lower lid lag with scleral show due to the excision of an excessive amount of lower eyelid skin. Such situations are solved with a skin graft. A lateral ectropion after canthoplasty is a potential but temporary complication.
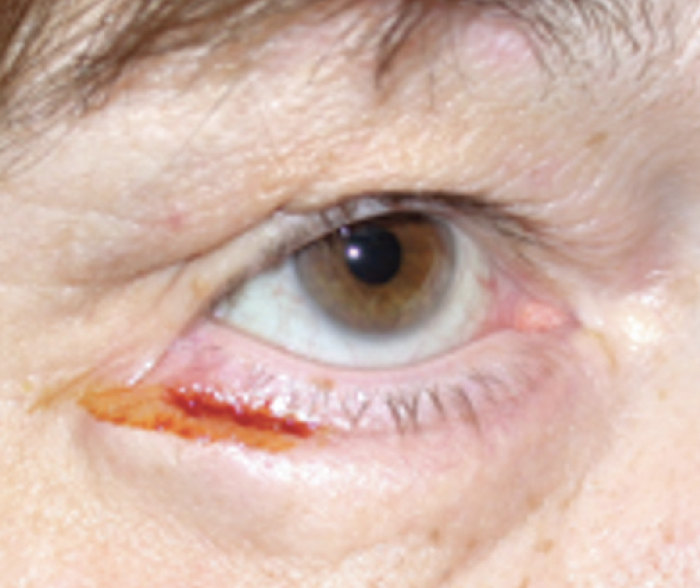
Figure 7. Wound dehiscence after a lower eyelid blepharoplasty.
CONCLUSION
Oculoplastics represents an area of growth potential for ophthalmology practices. Blepharoplasty can be a rewarding surgery when a thorough preoperative examination is performed, realistic expectations are set, and guidelines are followed. I find it effective to obtain photographs of patients 6 weeks after surgery and to allow them to compare these images with those taken preoperatively.
