


I prefer vertical chopping, preceded by some amount of preliminary sculpting. Using a vertical chop technique gives me more space in the anterior chamber, allowing me to perform chopping maneuvers further from the endothelium. Prior debulking of the nucleus also gives me access to a deeper nuclear zone that is easier to crack. Equally important, it gives me an idea of the strength of the zonules and firsthand information about the actual degree of nuclear sclerosis.
In my hands, I typically prefer a 30º standard phaco tip, but for very hard cataracts I prefer the Mega-Tip (Geuder). Both of these tips sculpt well and are also easy to occlude during chopping maneuvers.
Preliminary debulking can take the form of a crater or well (hemicrater; Figure 1), a short but deep trench, or a combination of the two depending on the type of nucleus. In ultrahard leathery cataracts, I like to create a long, deep trench (Figure 2). In other cases, a deep crater or well works just fine. Relatively high phaco power might be required for sculpting at this stage, in order to minimize inadvertent nuclear displacement and avoid zonular stress. Torsional phaco makes the sculpting process effortless. I also remove any fluffy cortical material near the rhexis margin to allow proper depth perception of the chopper tip and to avoid inadvertent trauma to the capsule.
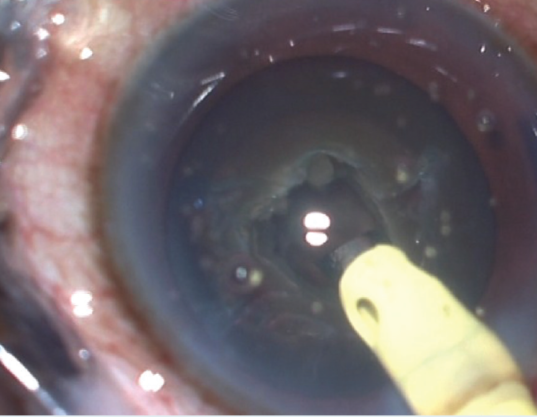
Figure 1. Preliminary debulking in the form of a hemicrater.
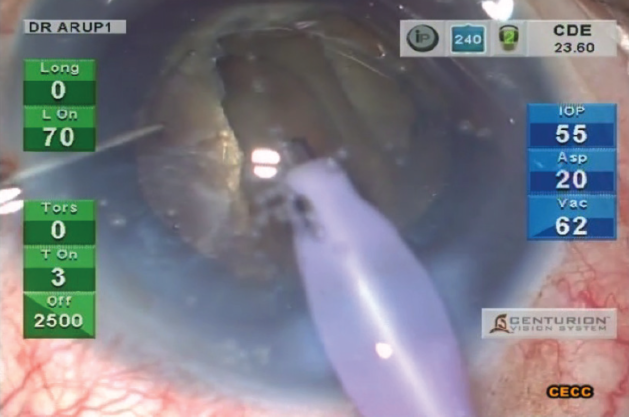
Figure 2. A long, deep trench created in an ultrahard leathery cataract.
I prefer vertical chopping to horizontal chopping because the former is more efficient and relatively faster in my hands. The distal tip length of most choppers is 1.25 to 1.5 mm, which should sufficiently reach the middle of a standard hard nucleus and create a reliable chop. A harder cataract, often about 5 mm thick, may call for the use of a chopper with a longer, sharp distal end of approximately 1.75 to 2 mm (Figure 3).
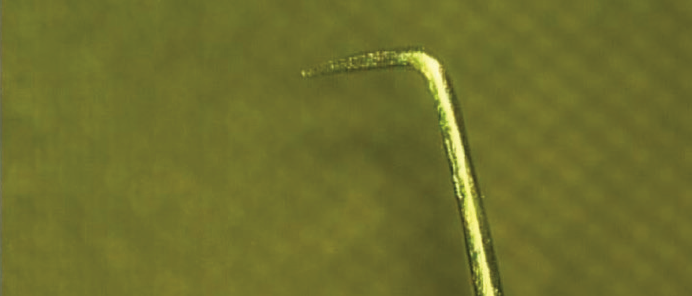
Figure 3. A long Chang chopper.
TWO VARIATIONS
Depending on the nature of the hard nucleus, I follow one of two variations of the chopping technique.
The brittle, hard nucleus. For a video demonstration of my technique in the brittle, hard nucleus, visit bit.ly/chakrabarti2_0517. After sculpting a deep well in the center of the nucleus, I use burst mode to impale the phaco tip at the deepest level of the nucleus. High vacuum is necessary at this stage for a good hold on the nucleus. The chopper is then buried deep into the substance of the nucleus, near the capsulorrhexis margin, and advanced toward the phaco tip.
I then proceed to crack or split the nucleus with lateral separation. I resist extreme degrees of lateral separation to minimize excessive stretching and distortion of the capsular bag and to avoid capsular-zonular complications. I then rotate the nucleus and repeat the same process until the nucleus is chopped into bite-size pieces. Keeping the tip bevel sideways (not advisable for Alcon Centurion Balanced tips) can provide extra endothelial protection and enhance visibility.
I realize the value of confining all these maneuvers entirely within the capsular bag and below the iris plane. Frequent replenishment of a dispersive OVD may be required for endothelial protection. Finally, care should be exercised by way of lowered parameter settings (vacuum, flow, and power) when removing the last piece of nucleus, as the posterior capsule is vulnerable.
The hard cataract with a posterior leathery nuclear plate. In these cataracts, I slightly modify my phaco maneuvers because the crack or chop line may not extend through and through in the first attempt and may inadvertently result in excessive lateral separation. This can jeopardize zonular integrity.
Here I sculpt a deep, long trench up to the rhexis margin before starting to chop the nucleus. Then I bury the phaco tip at the distal end of the groove before initiating the chopping maneuver. In this situation, I prefer to use the long Chang chopper (Rhein Medical). Keeping the phaco tip stationary, I then bury the chopper deep into the nucleus and move it obliquely toward the phaco tip before attempting the lateral separation maneuvers. If the chop line has not extended completely through the entire thickness of the posterior nuclear plate, I rebury the phaco tip into the nucleus at a deeper plane, just anterior to where the crack has extended, and repeat the same chopping technique until a full-thickness crack is achieved. In another Eyetube video (bit.ly/chakrabarti0517), one can see my surgical technique in a hard cataract with a posterior leathery nuclear plate. In this video, I use a Sinskey hook in place of the long-tipped Chang chopper, as this device can be daunting for the beginner.
WATCH IT NOW
Dr. Chakrabarti demonstrates his chop techniques in the brittle, hard nucleus and in the hard cataract with a posterior leathery nuclear plate.
Early removal of the first piece of nucleus may help to create more space in the bag so that successive subchopping maneuvers are easier. In hypermature cataracts, I prefer not to emulsify the subsequent nucleus pieces until the rest of the nucleus has been completely chopped, since it would empty the capsular bag, exposing the posterior capsule. The smaller nuclear fragments are then consumed using lower vacuum, flow, and power settings. As the chopping progresses, I exchange the long Chang chopper for a Sinskey hook once the first few pieces have been consumed.
It is also important to take care of the intraocular milieu in terms of protecting the endothelium and avoiding trauma to the incision for best outcomes.
In the presence of a hard cataract, my favorite chop techniques are stop and chop and direct chop. When the capsulorrhexis is large (about 6 mm) and the pupil dilates well, I prefer to do direct chop using high vacuum (550 or 600 mm Hg) with high pressure. If the pupil dilates poorly or the rhexis is small, I use stop and chop. With both techniques, I use the chopper to cut the nucleus as a means to reduce the use of phaco energy (Figure 4). In eyes with hard cataracts and concomitant pseudoexfoliation syndrome, I first try direct chop to put less stress on the zonula.
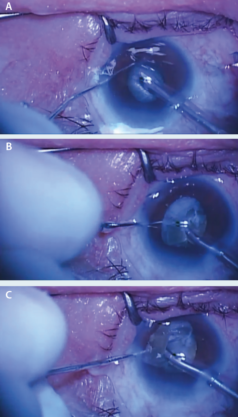
Figure 4. The chopper is used to cut the nucleus, reducing phaco energy in the eye (A–C).


