
Social Media Advertising Gives a Boost to Marketing
This approach is effective and cost-efficient.

By Arthur B. Cummings, MB ChB, FCS(SA), MMed(Ophth), FRCS(Edin)
The Wellington Eye Clinic participates in a number of studies, and, every now and then, we have to recruit patients for a particular study. Traditionally, this has been done through referral channels and public relations (PR) work, placing articles in newspapers and buying time on the radio. Recently, we were about to start another clinical trial that would enroll patients with mixed astigmatism who were interested in refractive surgery. We were getting ready, as usual, to spend money on TV and radio advertising that would invite patients to seminars to speed recruitment and make their initial examinations more productive.
Our PR agency lined up a top-flight advertising company to help us plan this drive. I was expecting to be pitched big-budget items including TV and radio slots. Therefore, I was pleasantly surprised when we were informed that this would not be productive nor provide much value for money. The ad agency was firmly of the belief that the best approach would be to advertise on social media, with Facebook specifically being the preferred route. Not only is this route cost-efficient, it is also effective, it can be specifically targeted at the right age group with the appropriate interests and hobbies, and it can be increased or stopped at the drop of a hat depending on how recruitment is going. Ads on social media can also provide digital links to the study information on the practice’s website, directly to the correct page.
This experience has changed my way of thinking about marketing in general. If social media advertising works best for driving recruitment for a study, then surely it will also provide the best return in routine marketing activities. Our experience to date is that this approach works just as well for the elderly as for the young. My children and the younger staff in the clinic tell me that Instagram and SnapChat are better than Facebook for reaching the younger generation, but we have not yet tried these two platforms for marketing purposes.
IN THE CLINIC
Once patients are in the clinic, the experience is much the same for all, young or old. We use Echo (Eyemaginations) to inform patients while they are waiting, and we have informational videos produced by our own practice that explain the procedures that we offer. The clinic’s website is practically laid out and navigable, so I always have it open when discussing options with patients. This way, all the relevant information is directly in front of us, beautifully presented and well laid out, and this assists me in spelling out the options as logically as possible.
I have the sense that younger patients have watched the informational DVDs that we send out more diligently than those in the older generation, but I may be mistaken about this. The informational DVD forms part of our consent process, so we insist that patients watch the DVD at least once. If they have not watched it before they arrive for their appointment, we show it to them in the clinic. While walking around the clinic from consulting room to consulting room, I notice that it is usually the older generation sitting behind the DVD players, while younger patients are using the free Wi-Fi and surfing the web while they wait to be seen.
INTERNET REFERRALS GROWING
The role of the Internet has grown enormously over the past 5 years. In 2010, word-of-mouth was responsible for 90% of our referrals, and the Internet about 7%. Today, word-of-mouth is around 72% and the Internet about 24%, meaning that Internet referrals have grown more than threefold in about 5 years.
Another trend is evident in the swing from PC-based applications to mobile-based applications. People engaging us via the Internet are now doing it mostly on smartphones, but also on tablets. It goes without saying that today’s websites must be mobile-ready, otherwise you will simply lose out on market share.
Practices Must Inform Both in Person and Online
Indiscriminate use of the Internet can sometimes give rise to confusion.

By Soosan Jacob, MS, FRCS, DNB
Communication, to me, still carries the classical meaning of an exchange between two people. For doctors, successful communication with patients requires several things. First, information must be simplified so that the patient can be aware of all of the options available to him or her. Second, the fears and apprehensions of patients and their companions must be allayed. Third, patients must be encouraged to learn more about their diseases and treatment options. In the office setting, these things are accomplished mostly in a verbal fashion, and, in the online world, through digital means.
FACE-TO-FACE
In the office, it is important to give as much time as reasonably possible to the patient. Patients must be allowed to speak first, in order to provide adequate background, and we must then discuss their problems with them. Because I head the department in a tertiary care hospital, patients generally come to me with all the required investigations done. However, if any are lacking, I ask for these to be performed as well.
Figure 1. Dr. Jacob’s YouTube channel.
I then spend time educating patients about their problems and the available methods to tackle them. It is important to let them know their options and the advantages and disadvantages of each. I generally find that a simple pen sketch helps most patients to understand easily. I also encourage patients to go to certain reliable sites on the Internet to find information to help them understand their diseases better. Finally, it is important to allow patients sufficient time to clarify all their doubts regarding their disease and their treatment.
DIGITAL INTERACTIONS
Face-to-face interaction in the office can be direct, personal, and tailored to each patient. Of late, however, many patients communicate with the doctor through electronic media, even before arranging an office visit. This communication can be in the form of emails, social media websites such as Twitter and Facebook, or comments posted on YouTube videos. Millennials use digital technologies much more than their elders. They are heavy users of social media, and these platforms offer good ways to reach out to them.
However, patients’ indiscriminate use of the Internet can sometimes give rise to confusion. Potential risks, even low risks statistically, may be enlarged disproportionately in patients’ minds. Therefore, these patients must be counseled more thoroughly and their fears must be allayed. In case of cosmetic and refractive surgeries, patients often must be counseled diligently to ensure that they have realistic expectations for the results of the surgery.
Digital communication provided by the surgeon or other members of the practice should aim to be scientific and precise. It can be offered online in the form of scientific blogs, webpages, social media, videos, and other platforms. I often find questions from patients on my YouTube surgical video channel (https://www.youtube.com/user/DrSoosanJacob; Figure 1), and this is a handy platform to help patients and answer their doubts. I can also add pictures and links to other informative videos.
Whether engaged in person or through digital media, a satisfied patient is your practice’s best ambassador.
Communication Changes in the Elderly
Adapt patient education strategies for those with hearing or visual problems.


By Simonetta Morselli, MD; and Antonio Toso, MD
Changes in communication abilities are commonly reported by the elderly. In a survey of more than 12,000 US Medicare beneficiaries aged 65 years or older, 42% reported hearing problems, 26% had writing problems, and 7% had problems using the telephone.1 Ophthalmologic patients are also affected by decreases of visual acuity, and, therefore, they have many problems with visual communication. They are not always able to use media, draw examples of what they are seeing, or access the Internet to understand their pathologies.
With typical aging, some language skills remain intact—for example, vocabulary, grammatical judgment, and repetition ability are relatively stable with age—while other skills tend to decline. Dual sensory loss (ie, decreased vision and hearing acuity) is increasingly common with age, especially in the very old and those in institutional settings. In a survey of people with dual sensory loss, more than two-thirds reported frequent difficulty in conversation, especially in noisy situations or groups.2,3 Poor hearing is often the cause of misunderstandings and negative reactions by communication partners, yet fewer than 24% of people who could benefit from hearing aids actually purchase them.4
Older patients normally are assisted during ophthalmologic examinations or surgery by younger relatives who are more skilled in communication. When we see an old, partially blind patient alone, it is difficult to explain what the pathology is and what the treatment will be. In these cases, we can use a lot of easy examples and simple words to explain the eye pathology. Sometimes these patients seem to understand, but oftentimes they tend to forget it all in a short period. In these cases, we often ask for a second consultation with a younger relative present in order to explain the situation better and to have a witness.
INTERNET FALLACIES
With the younger person accompanying the patient, we generally use digital communication to help us explain the proposed surgery or treatment. We normally use a laptop to show surgical or other types of videos in an attempt to explain the modalities of solving and caring for the patient’s pathologies. Some patients arrive in our office with incorrect opinions and mistaken so-called facts about their pathologies that they have found on the Internet, and they often are convinced of the efficacy of equally incorrect solutions to their problems.
Especially when we encounter young patients, it is difficult to overthrow their Internet-acquired points of view. This is the reason we use our own personal videos and other resources to counteract these erroneous sources and explain and instruct the patient in the correct point of view.
In our office, we have a digital system to collect videos and pictures at the slit lamp, and we always send relevant images to patients by email in order to correctly establish the pathology in the patient’s mind. Digital topographic analyses and digital fundus examinations can also be attached to patient emails. This is usually well appreciated.
CONCLUSION
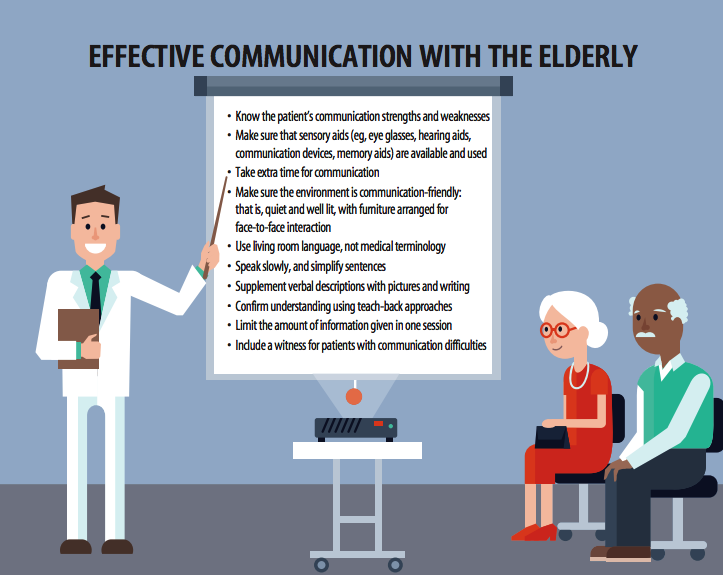
We try to customize communication with patients depending on their ages and attitudes, and this effort is generally well appreciated by our patients. We have a few communications tricks for dealing with elderly patients, which are detailed in the graphic on page 58.
Digital Media for Millennials and Boomers
Do we really need to differentiate?

By Karl G. Stonecipher, MD
How do you differentiate your market? What do you do differently to reach older and younger patients? The younger generation may need a slightly different twist than the older generation, but do we really have to change our course of action in marketing to millennials and baby boomers? I prefer, when possible, to use media that reach both older and younger patients. Remember, if grandma wants to stay in touch with her grandchildren, they all have to use some mutual platform.

Today, more important, both millennial and baby boomer generations are aware of the potential benefits of refractive surgery. In many cases recently, I have had grandparents who offer to pay for their grandchildren to have laser vision correction.
Any advertising option that works to reach both your cataract population and your laser vision correction population is media you want. One of my favorite advertisments for our practice was one that we placed in college newspapers several months before graduation season (Figure 2). This type of ad hits both populations, and when the parents or grandparents bring the child for surgery you can introduce them to your practice’s other offerings.
DIFFERENT WEBSITES
Having said all that, we do differentiate some of our marketing based on age. I have one website designed for an older population (www.lensdefinedvision.com) and another defined for a younger population (www.laserdefinedvision.com). We hand out business cards with the URLs for both web pages on them so patients and their family members can see what we do. We also use social media to keep in touch with both older and younger groups because I want everyone talking about what we do.
A TEXTABLE DOCTOR
I have also changed my course of action in the office. I do not always have time to check email until the end of the day or early in the morning. Therefore, I have become a textable doctor. One might think this would be a challenge, but really it makes my life easier. Whether it is an emergency postoperative issue or a mundane problem, it is the most important issue for that person at that time.
I constantly have people sending me selfies of their problems. Now, I point out to patients that this is really not “the next best thing to being there,” as the old Bell Telephone slogan said, but in many cases it allows us to resolve an issue without an office visit.
Before you decide to start doing the same, I would urge you to review the relevant laws for privacy and digital communication in your locality. It is likely that you need to document this patient encounter, even though it takes place through texting.
DIFFERENT STROKES
So remember, nowadays grandma and grandpa use text, Instagram, and Facebook, but they are not much on Twitter. The millennials really do it all.
1. Hoffman JM, Yorkston KM, Shumway-Cook A, et al. Effects of communication disability on satisfaction with health care: a survey of Medicare beneficiaries. Am J Speech Lang Pathol. 2005;14(3):221-228.
2. Heine C, Erber NP, Osborn R, et al. Communication perceptions of older adults with sensory loss and their communication partners: implications for intervention. Disabil Rehabil. 2002;24(7):356-363.
3. Heine C, Browning CJ. Communication and psychosocial consequences of sensory loss in older adults: overview and rehabilitation directions. Disabil Rehabil. 2002;24(15):763-773.
4. Garstecki DC, Erler S. Hearing in older adults. In: Shadden BB, Toner MA, eds. Aging and communication. Austin, Texas: ProEd; 1997: 97-116.
Arthur B. Cummings, MB ChB, FCS(SA), MMed(Ophth), FRCS(Edin)
• Consultant Ophthalmologist, Wellington Eye Clinic and Beacon Hospital, Dublin, Ireland
• Associate Chief Medical Editor, CRST Europe
• abc@wellingtoneyeclinic.com
• Financial disclosure: Consultant (Alcon/WaveLight), Chief Medical Officer (ClearSight Innovations)
Soosan Jacob, MS, FRCS, DNB
• Director and Chief, Dr. Agarwal’s Refractive and Cornea Foundation, Dr. Agarwal’s Group of Eye Hospitals, Chennai, India
• Senior Consultant, Cataract and Glaucoma Services, Dr. Agarwal’s Group of Eye Hospitals, Chennai, India
• Member, CRST Europe Global Advisory Board
• dr_soosanj@hotmail.com
• Financial disclosure: None
Simonetta Morselli, MD
• Head of the Ophthalmology Department, S. Bassiano Hospital, Bassano del Grappa, Italy
• Member, CRST Europe Editorial Board
• simonetta.morselli@gmail.com
• Financial disclosure: None
Karl G. Stonecipher, MD
• Director of Refractive Surgery, The Laser Center, Greensboro, North Carolina
• Member, CRST Europe Global Advisory Board
• stonenc@aol.com
• Financial disclosure: None
Antonio Toso, MD
• Consultant, Vitreoretinal Surgical Department, Ophthalmology Department, San Bassiano Hospital, Bassano del Grappa, Italy
• antonio.toso@gmail.com
• Financial disclosure: None