




In India and other developing countries, cataract surgeons continue to see a high number of rock-hard and brunescent cataracts.1 During the eras of extracapsular cataract extraction (ECCE) and manual small-incision cataract surgery (SICS), managing these cases was not a significant challenge, as the incisions used were large enough to accommodate the size of the nucleus, and, thus, cataract extraction was relatively easy.
AT A GLANCE
• Nucleus management in hard cataracts is more difficult with phacoemulsification than with ECCE or manual SICS.
• Risk of capsular-zonular problems and other collateral damage such as endothelial injury and wound burn increases in patients with brunescent cataracts.
• Comprehensive preoperative evaluation, surgical planning, slit-lamp examination, and documentation of the nucleus grade are key in these cases.
With the advent of phacoemulsification, nucleus management in hard cataracts has become more difficult. These nuclei require greater phaco energy for emulsification, and, as a result, the risk of capsular-zonular problems and other collateral damage, such as endothelial injury and wound burn, increases greatly.
In patients with brunescent cataracts, preoperative evaluation and surgical planning are of utmost importance. Careful slit-lamp examination and documentation of the nucleus grade are also important. Additionally, the surgeon must be aware of and prepared to address associated challenges that include zonular problems, lens subluxation, and small pupils. Capsular hooks, iris hooks, capsular tension rings, capsular tension segments, and a vitrectomy cutter should all be available as standby measures.
Phacoemulsification is best performed under topical anesthesia. However, depending on the surgeon’s confidence level, if the cataract is rock hard and brunescent and the surgical time is anticipated to be longer than usual, then a peribulbar block is preferred.
WATCH IT NOW
Below we share five fundamentals associated with the management of brunescent cataracts, which we believe can be useful to anyone attempting cataract surgery in these cases.

AVOID WOUND BURN
In hard nucleus cases, temporal clear corneal incisions (CCIs) are recommended. A beginner surgeon may opt to create a sclerocorneal tunnel incision with a 2.8-mm entry; this may help if conversion to manual SICS seems likely.

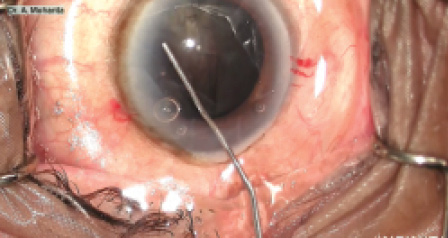
Figure 1. A 30° Kelman tip is preferable for initial nuclear sculpting.
Whatever incision site is chosen, wound burn is an important factor to keep in mind. Beginning surgeons may tend to be apprehensive and lift the phaco probe upward in order to avoid causing injury to the posterior capsule; however, this may indirectly cause harm, as the shaft presses against the roof of the incision with no fluid circulating in between, causing wound burn.
A slightly leaky CCI may help to cool the phaco tunnel from within. The surgical assistant can also put drops of balanced saline solution on the roof of the tunnel to keep it cool. The most significant causes of wound burn are a tight incision, because it increases frictional heat and hinders fluid flow; repeated OVD injection, which causes a no-flow state and subsequent wound burn; and a higher than usual energy requirement for emulsification of hard nuclear fragments.2,3
Wound burn typically appears as a well-defined chalky white patch on the upper lip of the tunnel. In particularly bad cases, a suture must be placed to seal the friable wound; typical wound hydration closure is not sufficient.
To prevent wound burn, ensure proper fluid flow around the tip of the phaco probe before applying power. The surgeon should remain in footpedal position 2, the irrigation/aspiration position, for some time until the occlusion sound stops, and then move to position 3 to deliver ultrasound power after proper fluid circulation has started.

PERFORM CAREFUL CAPSULORRHEXIS CREATION AND HYDRODISSECTION
In most cases with brunescent nuclei, lack of red reflex due to the density of the nucleus makes capsulorrhexis creation difficult. It is a good strategy to stain the anterior capsule with trypan blue dye to enhance visualization during this step. This is also helpful to prevent accidental damage to the capsulorrhexis, as good visualization can limit the risk of engaging the capsulorrhexis margin with the chopper tip.
The rhexis should be adequately large so that in the rare case of conversion to manual SICS or ECCE the surgeon can easily express the nucleus out of the bag. The capsule is sometimes quite thin, and the capsulorrhexis may extend uncontrollably to the periphery; once this occurs, the tear cannot be brought back, and in this event phacoemulsification becomes extremely dangerous due to the risk of nucleus drop.
The surgeon should be careful during hydrodissection, as the fluid wave is not clearly visible due to the density of the nucleus. Sometimes a capsular-lenticular block occurs, in which event the surgeon should target multiple points to inject irrigation fluid and decompress simultaneously in order to avoid posterior capsular blowout. Rotation of the nucleus is crucial before phacoemulsification, and it should be performed as gently as possible. The cortical capsular adhesions resist nuclear rotation, and forcible rotation can lead to zonular dehiscence.

LIMIT PHACO TIME AND POWER
Vertical chopping is preferred for nucleus division, as in brunescent cataracts the epinucleus is hardened and often inseparable from the nucleus. Horizontal chopping is not advisable due to the lack of space required to place the chopper at the lens equator. To better impale the ultrahard nucleus, retract the sleeve of the phaco tip about 2 mm to further expose the tip, and bury it in the nucleus deeper than usual. Care should be taken to avoid placing the irrigation ports inside the phaco tunnel to prevent chamber collapse.
Initial sculpting is used to weaken the core of the nucleus. This must be done with continuous power and low vacuum. A 30° Kelman tip (Figure 1) is preferable. Microburst mode is applied to impale the nucleus. At this stage, the vacuum should be high, between 450 and 500 mm Hg, in order to get a good grip on the nucleus.
A hard brown nucleus is about 4 to 4.5 mm thick. A sharp vertical chopper (Figure 2) with a 1.5 to 2 mm bend will penetrate deep into the nucleus and crack the posterior plate; this is not possible with a short, sharp chopper.4 With lateral separation force, the nuclear mass separates along the preexisting anatomic fault lines.4 The exposed tip of the phaco probe acts as a depth gauge.
If cracking is not achieved in one single go, multilevel chopping is employed—that is, the nucleus is impaled at a deeper plane before further employing lateral separation force. Too much lateral separation force and too many attempts to bring a large nuclear piece out of the bag may lead to zonular dehiscence.
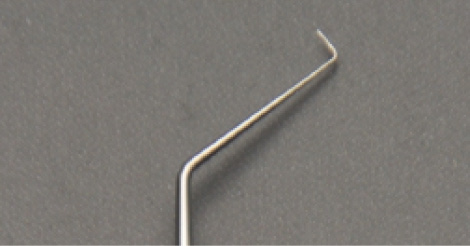
Figure 2. A sharp vertical chopper with a 1.5 to 2 mm bend can be used to penetrate deep into the nucleus and crack the posterior plate.
Because the removal of hard cataracts requires more phaco energy and phaco time, the surgeon’s aim should be to use the minimum phaco time and power possible. After the fragments are separated, they should be emulsified with one of the phaco technologies described below. The vacuum should be on the higher side to carry away the emulsate.
Hyperpulse technology. Hyperpulse and other pulse technologies reduce heat and energy production by using repeated on and off cycles. These pulse modes also reduce particle turbulence by increasing followability due to reduced chatter of fragments at the phaco tip.
Torsional technology. Torsional technology, such as the Ozil torsional handpiece of the Infiniti Vision System (Alcon), breaks up the nucleus with shearing force, not by the conventional jackhammer effect. Advantages of torsional phaco include increased followability, decreased energy use, shorter surgical times, reduced heat production, and less endothelial damage.
Intelligent Phaco. Intelligent Phaco is a software program on the Infiniti Vision System that delivers a small amount of preset burst energy when there is desired occlusion at the tip. This addition overcomes one minor disadvantage of torsional technology: tip occlusion. Intelligent Phaco greatly increases the efficiency of torsional phaco.
Once the hard nucleus is successfully split, it is sometimes necessary to further subdivide the fragments with additional chopping, as they may be oversized. This is best done with horizontal chopping.
Large, hard brown cataracts have large capsular bags. After some phacoemulsification is completed, the bag may tend to flutter and engage with the phaco tip during removal of the last quadrant, so extra caution must be taken during this step.

PROTECT THE ENDOTHELIUM
The reported average loss of endothelial cells after phacoemulsification varies between 4% and 25%.6 Crucial factors leading to endothelial damage include: (1) particle turbulence, (2) increased phaco power, and (3) tip occlusion by an OVD.
Use of an OVD comes into play to protect the endothelium, and these products are available in dispersive and cohesive types. Dispersive OVDs help protect the endothelial layer, whereas cohesive OVDs help create space. The soft-shell technique described by Steve Arshinoff, MD, is a useful method to protect the endothelium from particle turbulence. This technique maximizes the advantages and minimizes the disadvantages of both types of OVD by using these agents together. A dispersive OVD is injected first into the anterior chamber, followed by a cohesive OVD underneath the dispersive to create space, thus pushing the dispersive OVD toward the endothelium.7 This sequence may need to be repeated during surgery.

CONVERT TO ECCE OR MANUAL SICS WHEN NECESSARY
It sometimes becomes necessary to convert from phaco to ECCE or manual SICS because either the phaco energy consumption has exceeded safe limits or there is a capsular-zonular problem that cannot be managed in a closed chamber situation.
If conversion is required, the surgeon should enlarge the incision as in ECCE or convert to manual SICS. Multiple cuts should be placed at the rhexis margin, and the nucleus should be prolapsed into the anterior chamber and delivered out of the eye. If conversion to ECCE or manual SICS must be done once lateral separation is complete, leaving more than two or three fragments, the surgeon should be careful while delivering them, as these fragments can have sharp edges. Copious amounts of OVD should be used to protect the endothelium. One should keep a mental count of the fragments and be sure not to leave any in the eye, especially behind the iris plane, as these can cause further compromise.
As mentioned previously, if the surgeon is unsure of his or her own confidence in treating these cases, it is better to plan for ECCE or manual SICS rather than cause a posterior capsular rent or corneal decompensation later on. However, if the patient insists on undergoing phacoemulsification, it is best to refer him or her to a surgeon who can better handle the case with this approach.
CONCLUSION
Surgery in a brunescent cataract can be challenging, but, with the steps outlined here and with a little bit of confidence, any surgeon can handle them. One final note: It is imperative to always have a plan B ready while dealing with these cases.
1. Singh R, Vasavada AR. Phacoemulsification of brunescent and black cataracts. J Cataract Refract Surg. 2001;27:1762-1769.
2. [no authors listed] Scleral and corneal burns during phacoemulsification. Health Devices. 1996;25(11):426-431.
3. [no authors listed] Scleral and corneal burns during phacoemulsification with viscoelastic materials. Health Devices. 1988;17(12):377-379.
4. Kim HK. Decrease and conquer: phacoemulsification technique for hard nucleus cataracts. J Cataract Refract Surg. 2009;35:1665-1670.
5. Vasavada AR. Multilevel chop technique. J Cataract Refract Surg. 2011;37:2092-2094.
6. Walkow T, Anders N, Klebe S. Endothelial cell loss after phacoemulsification: relation to preoperative and intraoperative parameters. J Cataract Refract Surg. 2000;26:727-732.
7. Arshinoff SA. Dispersive-cohesive viscoelastic soft shell technique. J Cataract Refract Surg. 1999;25:167-173.
