

Presbyopia is a nearly universal disorder that will negatively affect us all at some point in our lives. Market Scope estimates that the number of people affected by presbyopia will continue to increase, reaching 2.1 billion worldwide by 2020.1 According to results of an online survey performed by Alcon and Jacksonville University, 49% of respondents would avoid reading glasses if they knew it made them look older, and 33% would seek an eye care professional if they knew there were remedies for presbyopia.2
AT A GLANCE
• A staged LASIK and Kamra inlay procedure can produce excellent visual outcomes; however, patient satisfaction can be tempered given the diminished UDVA from the MRSE of -0.75 and the requirement for two separate surgical sessions.
• Alternatively, a same-day combined LASIK and Kamra procedure can produce equivalent and excellent visual outcomes with greatly improved patient tolerance during the healing process and a reduced need for reading glasses in the early postoperative period.
• The combined procedure described in this article is technically more difficult for a number of reasons, and it should not be attempted until the traditional technique is mastered.
Numerous surgical approaches target presbyopia correction, including monovision laser vision correction, a variety of presbyopic LASIK approaches, and refractive lens exchange. These procedures function well for many people; however, all have the potential to affect visual quality through decreased contrast sensitivity, loss of stereopsis, and increases in halos and glare.3,4 The Kamra inlay (AcuFocus) has potential benefits over these and other approaches, but the candidacy requirements can be quite rigid.5
DETERMINING CANDIDACY
The Kamra inlay is approved for use in near-plano presbyopes who have a clear crystalline lens, have at least 500 µm of corneal tissue depth, and require a reading add of at least 1.00 D.5 The inlay functions through small aperture optics, increasing the functional depth of focus to approximately 2.75 D.5 As such, although nearly all patients will notice an improvement in depth of focus, patients who are slightly myopic at approximately -0.75 D will have the best combination of near and distance vision.5 This is illustrated conceptually in Figures 1 and 2.
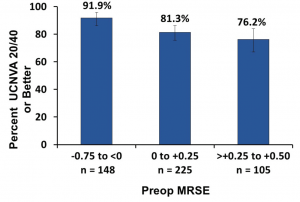
Figure 1. Improved near vision with myopic MRSE. (Data and figure obtained and used with permission from AcuFocus.)
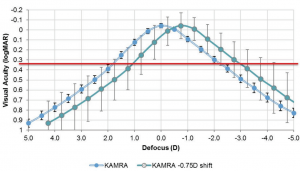
Figure 2. Defocus curves show improved depth of focus with -0.75 D shift. (Data and figure obtained and used with permission from AcuFocus.)
TRADITIONAL TECHNIQUE
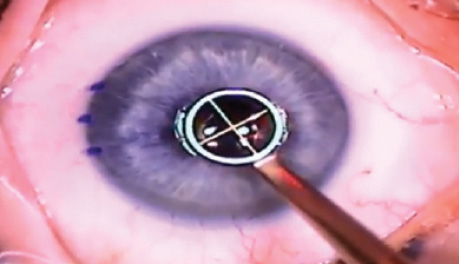
In early experience, the Kamra inlay was placed under a thick, LASIK-style flap. The inlay is now recommended to be placed in a pocket at least 200 µm from the corneal surface in the nondominant eye of a near-plano presbyope.6,7 The inlay is centered over the patient’s visual axis, where it blocks peripheral unfocused rays of light.5 The rationale for deep placement is that this should have less effect on the corneal nerve plexus and corneal biomechanics than shallow placement. Additionally, there is likely less inflammation and faster visual recovery given that there are fewer keratocytes deeper in the cornea.8
COMBINED TECHNIQUE
Because there are relatively few slightly myopic plano-presbyopes and because better visual outcomes are seen with the Kamra in those with a manifest refraction spherical equivalent (MRSE) of -0.75 D, I began performing a staged LASIK and Kamra inlay procedure on nearly all patients without previous ocular surgery.
In the beginning, I performed LASIK with a target of -0.75 D in the nondominant eye and plano in the dominant. The Kamra inlay was then placed on a subsequent day. This staged approach produced excellent visual outcomes; however, patient satisfaction was tempered given the diminished UDVA from the MRSE of -0.75 and the requirement for two separate surgical sessions.
To address this tempered patient satisfaction, I began performing a same-day combined LASIK and Kamra procedure. I have found this to be safe in my hands, and it has produced equivalent and excellent visual outcomes with greatly improved patient satisfaction. The procedure as I perform it is outlined in Same-Day Surgical Technique, and video of the surgery can be seen on Eyetube at http://bit.ly/rebenitsch916.
OUTCOMES
The Kamra inlay with the traditional approach has been reported previously to provide a mean binocular UNVA of approximately J2, which remains stable for at least 3 to 5 years.5,9,10 My experience with more than 50 Kamra inlays with the traditional approach has been at least equivalent to this.
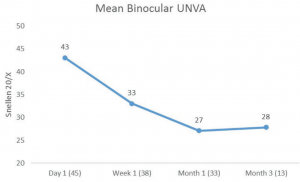
Figure 3. Mean binocular UNVA over time. The number of patients at each time point is shown in parentheses.
With the combined approach, I have found the same. I have performed the combined procedure in 48 patients, with postoperative results available for 33 at month 1 and for 13 at month 3. Three patients required next-day flap repositioning, which had no long-term sequelae. At 3 months, the mean binocular UNVA was 20/28. Monocular UDVA was 20/25, and binocular UDVA was 20/16. Mean monocular CDVA was 20/19. Improvement in binocular UNVA over time is shown in Figure 3.
CASE PRESENTATION
A 48-year-old man—an educator—presented to our clinic with a 3-year history of difficulty with near tasks and no significant ocular history. On exam, his UDVA was 20/30 OD and 20/25 OS. Manifest refraction was 1.00 D sphere OD and 0.75 D OS; cycloplegic refraction was the same. Slit-lamp examination showed a healthy cornea with a good tear film, a clear lens, and a healthy fundus in each eye. Corneal tomography showed no irregularities, with pachymetry of 525 µm OD and 535 µm OS.
The patient was recommended to have LASIK in his dominant right eye and combined LASIK and Kamra inlay in his left. The procedure was performed with targets of plano OD and -0.75 D OS. Visual recovery was as follows:
Day 1: UDVAs, 20/20 OD, 20/25 OS; binocular UNVA, 20/40
Day 10: UDVAs, 20/12 OD, 20/20 OS; binocular UNVA 20/25
Month 3: UDVAs, 20/16 OD, 20/20 OS; binocular UNVA, 20/25.
The patient is now 6 months postoperative and satisfied with his distance and near vision without eye dryness or visual disturbances.
CLINICAL PEARLS
The combined procedure is more technical for a number of reasons, and it should not be attempted until the traditional technique is mastered. An opaque bubble layer can obscure visualization. The surgeon must ensure that the flap edge and entrance to the pocket do not intersect. Flap displacements can occur, and they must be addressed.
Watch it Now
In my experience, most presbyopes become satisfied with the procedure when their binocular UNVA is 20/30 or better. Monocular UDVA must also be 20/30 or better. This can occur as early as the next day, but in some patients, can require months. Effective lubrication of the ocular surface is paramount, as nearly all patients will suffer from eye dryness for at least the first few months.
I have also found that, although distance vision is important, near vision is even more so. As a result, when planning the target for the Kamra eye with LASIK, I tend to aim for a target of -0.75 to -1.00 D rather than -0.50 D, which would be well within the approved MRSE for the inlay. With this targeting strategy, patients have been better able to avoid reading glasses throughout the normal fluctuations during the healing process.
Patients must be counseled on the need for patience with this procedure, as vision improves over months rather than days and can fluctuate for up to 9 to 12 months in some. The visual results are excellent, but the recovery is not as fast as with other forms of laser vision correction. What we have found with the combined procedure, however, is that, given an ideal MRSE outcome, tolerance during the healing process is much greater. The need for reading glasses in the early postoperative period has been greatly lessened as a result.

CONCLUSION
The same-day LASIK and Kamra inlay procedure has been effective in our practice, greatly improving patient satisfaction.
1. Market Scope. Global Presbyopia-Correcting Surgery Market Report. April 2012.
2. Alcon study reveals nearly half of Americans would avoid reading glasses if they knew it made them look older [press release]. Alcon, May 15, 2015. https://www.alcon.com/news/media-releases/alcon-study-reveals-nearly-half-americans-would-avoid-reading-glasses-if-they. Accessed August 3, 2016.
3. Durrie D. The effect of different monovision contact lens powers on the visual function of emmetropic presbyopia patients (An American Ophthalmological Society Thesis). Trans Am Ophthalmol Soc. 2006;104:366-401.
4. Chang JS, Ng JK, Lau SY. Visual outcomes and patient satisfaction after presbyopic lens exchange with a diffractive multifocal intraocular lens. J Refract Surg. 2012;28(7):468-474.
5. Brown JN. P120023 Kamra Inlay. Presentation to FDA advisory committee. June 6, 2014. http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/MedicalDevices/MedicalDevicesAdvisoryCommittee/OphthalmicDevicesPanel/UCM400433.pdf. Accessed August 3, 2016.
6. Jalali S, Aus der Au W, Shaarawy T, et al. AcuFocus corneal inlay to correct presbyopia using femto-LASIK. One year results of a prospective cohort study. Klin Monbl Augenheilkd. 2016;233(4):360-364.
7. Tomita M, Waring GO 4th. One-year results of simultaneous laser in situ keratomileusis and small-aperture corneal inlay implantation for hyperopic presbyopia: comparison by age. J Cataract Refract Surg. 2015;41(1):152-161
8. Patel S, McLaren J, Hodge D, et al. Normal human keratocyte density and corneal thickness measurement by using confocal microscopy in vivo. Invest Ophthalmol Vis Sci. 2001;42(2):333-339.
9. Dexl AK, Jell G, Strohmaier C, et al. Long-term outcomes after monocular corneal inlay implantation for the surgical compensation of presbyopia. J Cataract Refract Surg. 2015;41(3):566-575.
10. Yilmaz OF, Alagoz N, Pekel G, et al. Intracorneal inlay to correct presbyopia: Long-term results. J Cataract Refract Surg. 2011;37(7):1275-1281.
R. Luke Rebenitsch, MD
• Refractive Surgeon, ClearSight Center, Oklahoma City, Oklahoma
• Dr.Luke@ClearSight.com
• Financial disclosure: Lecture fees (AcuFocus)
