



On Sunday, October 25, 2015, I returned to the United Kingdom from Washington, DC, where I had been invited to give a guest lecture to the annual meeting of the Retina Group of Washington (http://rgw.com). It was a daytime flight, and I arrived home late that night, exhausted. I went straight to bed, as I had surgery planned the next day.
At 4 am, my phone rang. It was the key-holding company for my private practice; they had been called out because our intrusion alarm had gone off. They told me that they had entered our building in East Grinstead, and one-half was completely flooded, with water coming down through the ceilings. They said I had to get a plumber in as soon as possible to turn off the main water supply.
I was not sure if I was having a bad dream! I logged into the closed-circuit TV system we have at the office. Most of the channels were dark because it was the middle of the night and no lights were on. On the waiting area camera, however, I could see a discoloration on the carpet that was gradually expanding.
I spent the next 1.5 hours trying to find a plumber—I could not believe how difficult it was to find an emergency plumber at that time of the morning. All the ones advertised on Google either did not answer or told me that they could not do the job because they had no one to attend to the problem. I finally got hold of someone who was keen to do the job, and I arranged to meet him at the center, which is a 45-minute drive from my home.
By the time I got to the practice, the fire brigade was already there, and the plumber had managed to turn the mains off from a hydrant in the road. The fire brigade turned off the electricity supply to prevent electrocution and fire. They were reluctant for me and my staff to enter the area that had been flooded, as there was a possibility of the ceiling collapsing—which eventually happened.
WHAT NEXT?
Soon after I got there, our Director of Operations, Gael Ogunyemi, also arrived. Together we walked through the building to assess the extent of the damage. Our laser suite, OR, and sterilization facility (UK regulations require four rooms) were all completely flooded (Figure 1). Water from a burst pipe had come through the ceiling in multiple locations (Figure 2), and our most expensive items, including our excimer laser, our IntraLase femtosecond laser (Johnson & Johnson Vision), and our Victus femtosecond laser (Bausch + Lomb) , were damaged. Stock items including lens banks were a write-off, as was our phaco machine. The sterilization facility was not useable.
Shortly thereafter, Gael, I, and other key individuals at our organization met in a boardroom upstairs to work on an action plan to get us through the problem. We had patients due for surgery that day, and we also needed to plan for the future. Keeping absolutely calm, we mapped out an immediate plan to see the business through and began to consider the steps needed to repair the building (Figure 3).

Figure 1. Damage extended into the laser suite, OR, and sterilization facility.

Figure 2. Water from a burst pipe had come through the ceiling.
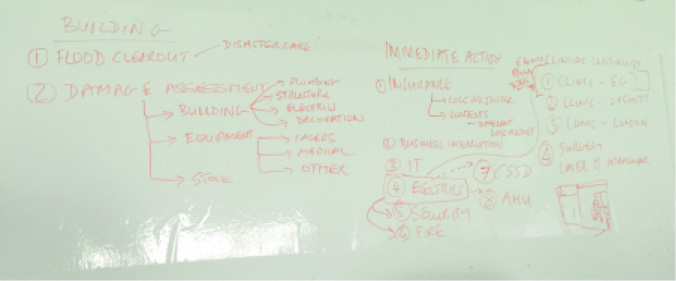
Figure 3. An initial strategy was mapped out within hours after the disaster.
Fortunately for us, 3 weeks earlier, we had modified the ventilation system at our other facility in Surrey, a 45-minute drive away and equipped ourselves to perform intraocular surgery there. We had already been doing laser eye surgery there for a couple of years, and, although we had the one surgical facility already, I always felt a little vulnerable not having an alternative location. What if we had VIP patients who had travelled internationally, and a laser or other key device broke down? With increasing interest in refractive lens exchange among our patients, it made sense to add intraocular surgery at that other facility.
It was clear to us that it would take at least 3 to 4 months to dry out the damaged facility and get it back to operational status. As local private hospitals would not be able to cope with our volume, and as the cost to use the hospital facilities would be prohibitive, our only option was to make use of our Surrey facility. We planned accordingly, knowing there would be fallout with some patients being unwilling or unable to travel.
We also had to ensure that our reputation was not damaged as a result, and we resolved to do whatever it would take to limit reduction in referrals. It is very easy to lose business and much harder to gain it back.
THE RESPONSE
The response and support we received from the ophthalmic industry was fantastic. Most of our biggest vendors had representatives onsite at our facility the same day. Although they tried to do what they could to limit the damage, they were unable to do so. They did, however, provide considerable support and offered to assist in any way possible at our other site.
There were numerous aspects to getting back up and running that we had to deal with, and these were ably managed by Gael. Restoring the building took longer than expected: It took 3 months just to dry out—and 7 months to become partially operational (Figure 4).

Figure 4. After the damaged areas in Dr. Daya’s clinc were cleared of water and debris, the undamaged areas were taped down so that the practice could maintain partial use of the clinic.
Poor Gael struggled with two different insurance companies and a loss adjuster to have the building dried out and refurbished. We were bound by our insurance policies, with the rate-limiting factor being one representative at one insurance company who had no sense of urgency. We were concerned that, if we initiated and funded the expensive repairs ourselves, we would not be reimbursed by the insurer.
We also discovered that business interruption has many effects that are not always initially identifiable, and it ultimately affects the bottom line. We sought the assistance of an expert claims consultant and finally managed to get a fair sum repaid for loss of business.
Because all of our lasers had to be replaced, along with all the other flood-related issues, the claim exceeded £3 million. Understandably, the insurance company was determined to claim this in turn from the company that maintained our mechanical and engineering systems in the building.
In order to renew our insurance policy, we were expected to establish systems to prevent a future flood. We had multiple water sensors placed in areas where water might leak. The sensors are linked to our mechanical controls, and, in the event that water is detected, the mains supply of water will be shut down. This is a great idea, and I’m not sure why homes and buildings are not routinely built with these kinds of systems already installed.
We came through this disaster without losing our business and practice mainly because we had an alternative facility available for use and because the whole project of maintaining the business and rebuilding was well managed by our director of operations, to whom we express our tremendous gratitude.
WHAT DID WE LEARN?
The silver lining, if there is one, is that we learned a number of lessons in the course of dealing with this disaster:
No. 1: The value of staying calm. This is easily said, but it is quite possible that panic will take control in the face of a crisis; the end result is that the situation might not be managed well. In our circumstance, good leadership, taking a calm and systematic approach, and involving all parties in developing a strategy to get through the crisis were very beneficial.
No. 2: Staff members are equally concerned about the impact of the problem on the business and, ultimately, their own positions. I personally found gratifying the involvement and support of staff members who made considerable contributions during our disaster and who went the extra mile to help keep things on track.
No. 3: Managing risk—although it sounds like business- speak—is a vital process that is worth conducting on a regular basis. Risk covers many aspects and is a large topic in itself.
No. 4: Have an action plan for each area of risk. For instance, have a list of emergency numbers for those who can provide services at short notice. Document the location of vital services and how they can be controlled.
No. 5: Be sure that every aspect of your practice, including business interruption, is well insured. Read over your policies carefully, and develop a good relationship with your broker. Make sure that he or she understands your practice, your business, and your needs. In particular, make sure that there are no gaps between buildings insurance and contents insurance. It makes sense to have both policies under one insurance company, to help eliminate gaps and grey areas.
No. 6: Make use of experts. Although the insurance company will provide a loss adjuster, it is best to hire an independent adjuster to look after your own interests. We benefited considerably from our independent agent, who identified areas of loss and a rationale for claims that we had not initially considered.
No. 7: Good relationships are invaluable. Although this is something that has mattered to me for the entirety of my 25-plus years in practice, it was clear that our partners in the ophthalmic industry provided considerable support on many fronts to help us get through the crisis. We are indebted to the industry, in particular to the relationship managers at Bausch + Lomb and Johnson & Johnson Vision.
CONCLUSION
I would not wish anything like this on anyone, and I hope that this story helps readers work toward considering risk and its impact. I learned a great deal after going through this episode, and I am thankful to be able to continue in practice. Although we had a drop in business after the incident, we are now back on track again.
