



One of the most important aspects of successfully performing small-incision lenticule extraction (SMILE) is mastering a refined docking technique. Although SMILE is performed in just one step, achieving excellent refractive results requires a thoughtful preoperative protocol for docking the femtosecond laser.
This article constitutes my dock talk, an outline of the steps to implement when the patient is under the microscope and the laser-focusing cone is fully calibrated and ready to fire.
AT A GLANCE
- Although small-incision lenticule extraction is performed in just one step, achieving excellent refractive results requires a thoughtful preoperative protocol for docking the femtosecond laser.
- It is important to speak calmly to the patient during fixation and energy delivery.
Five crucial steps
No. 1: Place the lid speculum in the eye to be treated. This should be done in conjunction with step No. 2 (below).
No. 2: Position the patient’s head. His or her face is parallel to the floor, or his or her chin is slightly elevated from that position. This positioning provides full exposure and ensures that the upper eyelid does not block the laser focusing lens from centering on the cornea.
No. 3: Angle the patient’s nose. Adjust the patient’s head so that his or her nose tilts away from the focusing lens (Figure 1). Ideally, the nose will be at the 11-o’clock position, head tilted slightly to the left for the right eye or slightly to the right for the left eye. This positioning will prevent the focusing lens from hitting the patient’s nose when you bring down the lens to contact the cornea. Otherwise, the patient’s nose may block the laser-focusing lens from fully applanating the cornea.
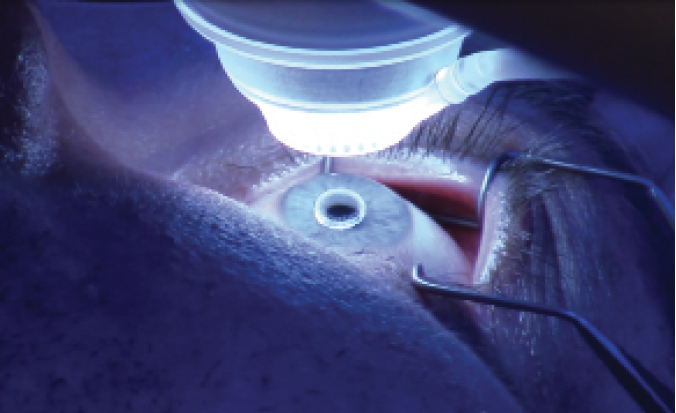
Figure 1. The lid speculum is in place, and the patient’s head has been tilted so that the nose is rotated away from the focusing lens.
No. 4: Verify fixation. At this point, the patient should be looking at the fixation light (Figure 2). Confirm that he or she sees it. Explain that the SMILE procedure is not a difficult experience, but advise the patient to expect to feel pressure and note that it is a normal and weird sensation but a tolerable one. Tell the patient that a time will come, while he or she feels some pressure, when his or her vision will dim as the focusing light blurs and disappears. Emphasize that the patient should stay relaxed during this moment. For example, I might say, “For the next 30 to 45 seconds, I am going to ask you not to move your hands or feet, not to let your chin drift up or down, and not to look around with your eyes. Simply be still.” Ideally, you will have reviewed these instructions with the patient preoperatively as well.

Figure 2. The patient is instructed to look at the green fixation light during docking.
No. 5: Move the focusing lens. Now that the patient is calm and knows what to expect, pull the focusing lens down close to the cornea while reminding him or her to look at the blinking green fixation light (Figure 3). I recommend using both of the words blinking and green in case the patient is color blind.

Figure 3. As the focusing lens comes into contact with the cornea, the patient is reminded to look at the blinking green fixation light.
While the patient fixates on the light, I watch the pupil as I use the joystick to lower the focusing lens onto the cornea. The goal is for the center of the pupil to be the first place the focusing lens touches the cornea.
If the focusing lens is not on the center of the pupil, double-check that the patient is looking at the fixation light. If he or she is still looking at it but the focusing lens is not centered, readjust it with the joystick while reminding the patient not to look away from the focusing light. If the readjustments are not getting you closer to the center of the pupil, check to see if the cone is touching the patient’s nose. If it is, tilt the patient’s head away from the focusing lens a bit more so that his or her nose does not hit the cone.
When you are happy with the centration, bring the focusing lens down so that 80% to 90% of the applanation is occurring. Then, press the suction button located on the top of the joystick, at which point 100% applanation should occur. If full applanation does not happen immediately, quickly turn off suction, move the focusing lens down a bit farther for more applanation, and then press suction again. When you have full applanation, remind the patient not to worry about the pressure, and instruct him or her to avoid talking. It is important to speak to the patient calmly during energy delivery, to remind him or her repeatedly not to talk or move, and to provide assurances that everything is going great.
Expanding the Pool of Candidates
By Steven C. Schallhorn, MD

In the United States, small-incision lenticule extraction (SMILE) is approved for the treatment of patients with -1.00 to -8.00 D of myopia, -0.50 D or less of cylinder, and a manifest refraction spherical equivalent of -8.25 D. My fellow researchers and I conducted a straightforward analysis of the preoperative sphere and cylinder in patients who underwent LASIK and met the aforementioned criteria for SMILE. Presented at the SMILE user group meeting held by Carl Zeiss Meditec in New Orleans in November 2017, our findings suggest that SMILE should be applicable to a higher percentage of laser vision correction candidates than originally thought.
OUR FINDINGS
Our retrospective analysis involved a large cohort of previous LASIK cases. The purpose of the study was to assess the potential suitability of SMILE for patients with 1.00 D or more of myopia. The study included 55,461 eyes of 29,677 patients who met the full refractive sphere and age range (22–60 years) specified for SMILE but not the cylinder (manifest astigmatism, 0.00 to -6.00 D) before their LASIK procedure. Patients’ average age was 35 years.
Of all the LASIK patients whose preoperative parameters were within the age and sphere indications for SMILE, 43% had 0.50 D of manifest astigmatism or less in both eyes. Equally important, 19.7% of the total LASIK patients had manifest astigmatism of 0.25 D or less in both eyes. These results indicate that a higher percentage of patients than previously thought may be eligible to undergo SMILE within the currently approved range.
Next, to better understand SMILE’s outcomes in patients with up to 0.50 D of preoperative astigmatism, my colleagues and I reviewed the satisfaction surveys of participants in the FDA clinical trial that led to the procedure’s approval in 2016. Postoperatively, 329 patients completed a questionnaire as part of the pivotal clinical trial.
Our study analyzed three different aspects of satisfaction: need for glasses or contact lenses to improve postoperative vision, willingness to have the surgery again, and overall satisfaction with the outcome. We reviewed the results for the three preoperative manifest cylinder groups: 0.00, 0.25, and 0.50 D. We found that, 6 months postoperatively, there was no difference in patient satisfaction across these cylinder groups (Figure 1).
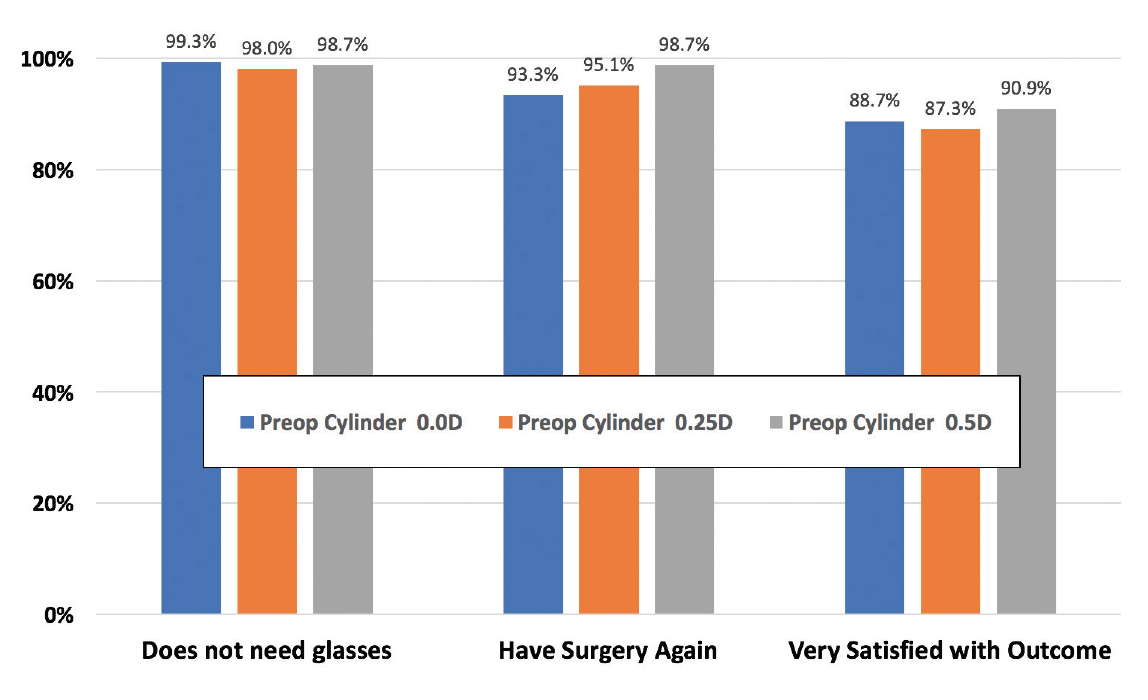
Figure 1. Patient satisfaction 6 months after SMILE.
CONCLUSION
The results of our analysis should give refractive surgeons a measure of confidence in considering SMILE for patients who have 0.50 D of preoperative astigmatism and meet the other indications for the procedure.
Likewise, the approved SMILE parameters should be applicable in up to 40% of myopic patients who seek refractive surgery and otherwise meet the indications for LASIK.
CONCLUSION
Proper docking and centration during SMILE are paramount to the procedure’s success. I find that the steps outlined here have greatly reduced the chance of problems such as a suction break during the laser treatment.
