


It is important not to underestimate the difficulty of removing a soft nucleus. And it is important to understand that we are likely to be faced with more and more soft nuclei in the future, for two reasons.
First, I believe that, as IOL technology advances, and features such as trifocal and extended depth of focus optics become increasingly available, younger patients with early cataract may become interested in elective cataract surgery. These patients will have softer nuclei than the traditional older cataract patient (Figure 1).
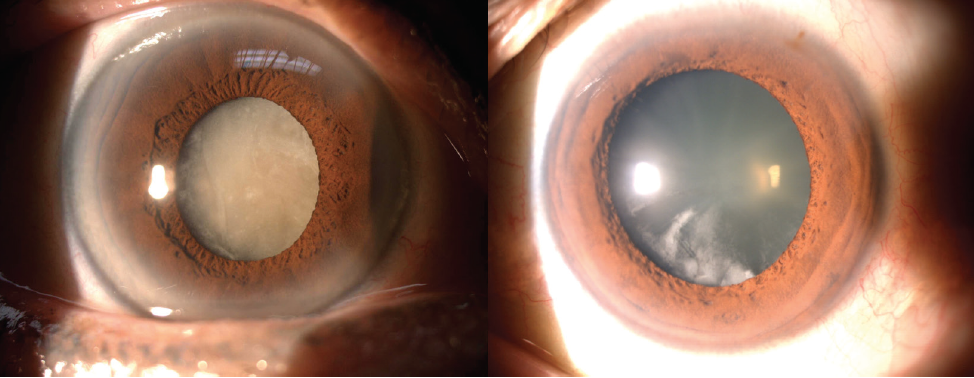
Figure 1. Young RLE or early cataract patients (right) have softer nuclei than traditional older cataract patients (left).
Second, lens-based refractive surgery via refractive lens exchange (RLE) is likely to account for a larger share of comprehensive refractive surgery in the coming years, and in these young patients, likely around 50 years old, we may encounter very soft lenses, for which we will perform near-clear lens extraction. We must weigh the risks of posterior capsular rupture (PCR) and other potential iatrogenic complications when we perform cataract surgery in these quite healthy young eyes.
In this article I outline five main considerations to have in mind when planning and performing lens surgery on soft nuclei.
1. CHANGING EPIDEMIOLOGY
Why are we even discussing soft cataracts? In the past, surgeons typically performed cataract surgery only in eyes with mature, hard cataracts, and experience with soft cataract removal was limited. With the trend toward RLE and refractive cataract surgery, surgeons are now performing cataract surgery more often on younger patients who desire spectacle independence.
Soft grade 1+ nuclei have always challenged us, but in the past we mostly avoided the challenge because relatively few patients sought early cataract surgery. Now, it has become vital to know how to handle this presentation, as the availability of improved technology and awareness of the option of RLE as a form of refractive surgery brings more younger patients to our practices.
2. DETERMINING NUCLEAR HARDNESS
When we examine patients before cataract or RLE surgery, we must determine the level of nuclear hardness and note this in the patient’s record. This information allows us to plan for lens surgery in the most efficient manner. No matter what system we use—the Lens Opacities Classification System III (LOCS III), the subjective rating of nuclear sclerosis (NS) from 1+ to 5+, or simply calling the nucleus soft or hard—we need this information to guide us later in the OR.
It should be noted that, in addition to soft and hard nuclei, in young people, we are often faced with what I call the neither-here-nor-there (NHNT) lens. The NHNT lens is not soft enough to simply aspirate and not hard enough to crack or chop without taking extra precautions. This is the lens that is probably the most challenging for surgeons because it is … neither here nor there.
3. FACING CHALLENGES
The main challenge in the soft or NHNT lens is completing nuclear division to allow safe and efficient removal of the lens tissue.
The soft lens offers no resistance to pushing forces, making it difficult to rotate or to crack. It is also difficult to grasp by occluding the phaco tip. There is a tendency for the phaco tip to core through the lens rapidly, endangering the posterior capsule.
All of these characteristics make the basic, familiar steps of nucleus removal more challenging. We are used to hydrodissecting the nucleus, cleaving it from the epinucleus and cortex and allowing lens rotation and manipulation. We need to be able to do these things in order to crack or chop. But in trying to rotate the soft nucleus, we find that the instrument goes right through the nucleus instead of pushing and rotating it.
Similarly, when we crack a hard nucleus, we push apart the two halves to try to separate and crack the nucleus down to the base, but, in the soft nucleus, the instrument goes through the tissue.
Gripping the nucleus is also a challenge. When we activate the footpedal for suction to grip, as we would in a hard nucleus, the phaco tip can go right through because the nucleus is so soft—and before we know it we are at the posterior capsule.
4. MANAGING COMPLICATIONS
The main complication we encounter when dealing with a soft nucleus is PCR. This is related to the amount of force we apply to the nucleus. If we put too much force on the soft nucleus, the phaco tip goes right through the nucleus and toward the capsule, and if ultrasound is engaged when the tip hits the capsule, there goes the capsule.
This is a real risk of surgery in these young patients. If we rupture the capsule in a young person who had only a mild cataract, or one who was expecting to achieve better vision in his or her healthy young eyes after RLE, we face a difficult discussion with that patient postoperatively. It is hard to explain to patients who come to you just to get better vision that there has been a complication that will affect outcomes or will require additional surgery.
It is wise to set reasonable expectations for these patients preoperatively and to have an earnest conversation around informed consent to ensure that they truly understand that there are significant risks involved in intraocular surgery.
5. DEVISING TECHNIQUES
If we encounter a NHNT lens, we must have NHNT techniques available to safely remove it. I have three approaches that I use to free and mobilize the soft nucleus.
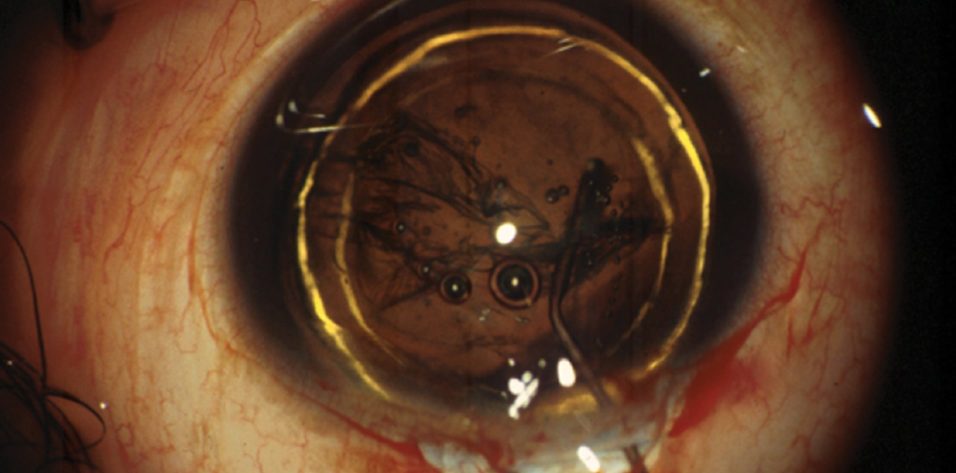
Hydrodelineation and en bloc removal. Hydrodissection alone, as we would perform in a hard nucleus, leaves a big messy lump of mixed cortex, epinucleus, and nucleus. Instead, I favor performing hydrodelineation just around the nucleus, resulting in the well-known golden ring (Figure 2). This step isolates the nucleus, allowing easy en bloc removal with vacuum only.

Figure 2. Hydrodelineation, resulting in the golden ring, can allow en bloc removal of the nucleus.
Modified stop-and-chop. Sometimes we do a modified stop-and-chop maneuver in NHNT nuclei. As noted previously, in these eyes there is no resistance to pushing forces, it is difficult to occlude and grip the nucleus, and there is a tendency for the phaco tip to core through rapidly. We don’t have the luxury of time, waiting to grip the nucleus to chop. The surgeon must form a deep, narrow groove, keeping in mind that impaling may core through the nucleus, and perform a quick, vertical chop as soon as the phaco tip begins to engage the nucleus.
Prechop. Another approach is to perform a prechop maneuver, either as an element of laser cataract surgery or as a manual karate prechop technique. Either method divides the nucleus and allows easy removal.
CONCLUSION
Overall, it is vital to assess nuclear hardness as part of the preoperative assessment and then to match your surgical technique to the nuclear density.
For very soft nuclei—say, in patients under age 30—we can usually simply aspirate the nucleus without any use of ultrasound at all. Patients in their 40s and 50s are more likely to have NHNT cataracts, and for these patients it is best to adopt one of the techniques described here, either prechop or hydrodelineation and en bloc removal. If the cataract is on the harder side of soft, the stop-and-chop technique may be preferred, but it must be modified to a quick vertical chop.
When I go to the OR, I have a note in my list telling me the nuclear density for each patient so that I know what I will be facing. This is the best way to avoid complications in these deceptively difficult soft and NHNT nuclei. So plan ahead, counsel your patients well, and beware the NHNT cataract.



