



This story began in November 2015, when two sisters, each intolerant of progressive multifocal spectacles, presented with hyperopia, astigmatism, and good BCVA. Their ocular and physical health was similar. Their refractions are depicted in the graphic below.
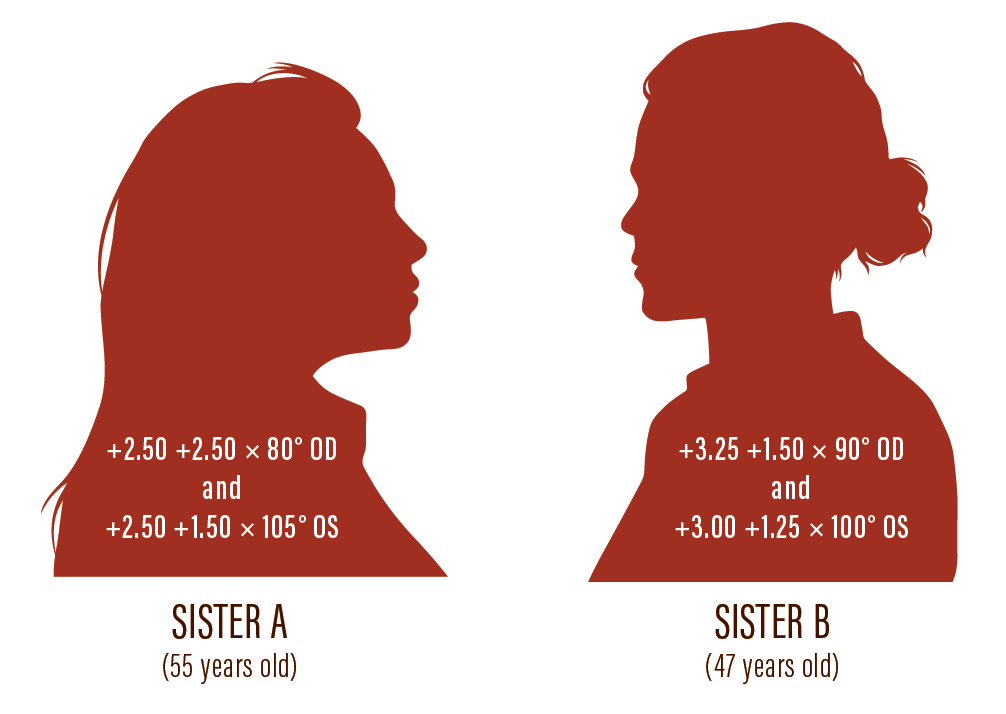
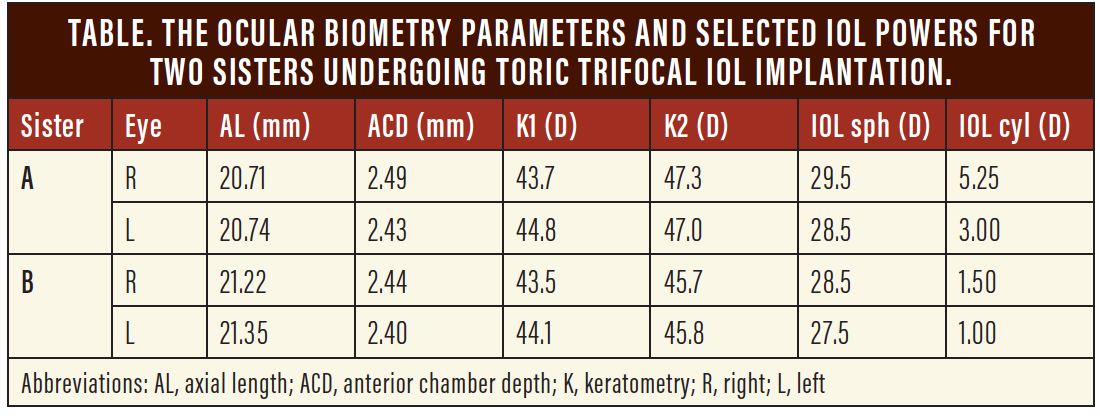
Because both women desired spectacle independence, and because their anterior chamber angles were narrow (posing some risk for angle-closure glaucoma), I suggested that they each undergo refractive lens exchange with trifocal toric IOL implantation (Pod FT, PhysIOL). Preoperative anterior corneal topography with the Aladdin (Topcon) showed regular astigmatism and no evidence of forme fruste keratoconus. The ocular biometry parameters and the selected IOL powers can be found in the Table.
At the patients’ request, they each underwent same-day sequential cataract surgery. The younger sister’s surgery was performed 2 weeks after the elder’s. All four surgeries were uneventful.
POSTOPERATIVE Outcomes
One month after the surgery, refractive and visual outcomes for both patients were incredibly positive. Refraction showed only some residual myopic astigmatism, less than 0.75 D. Binocular uncorrected distance visual acuity (UDVA) was 0.02 logMAR for Sister A and 0.00 logMAR for Sister B. Binocular uncorrected near visual acuity was J2 in both sisters.
Each sister experienced photic phenomena—halos, glares, and starbursts—due to the diffractive lens design, which they had been counseled preoperatively to anticipate. However, they also reported disturbing peripheral arcs of light that I had not mentioned before surgery. Sister A was particularly upset about this unexpected positive dysphotopsia, and I spent several postoperative visits attempting to convince her to wait for the symptoms to subside. She made the drawing shown in Figure 1 and repeatedly asked for solutions.
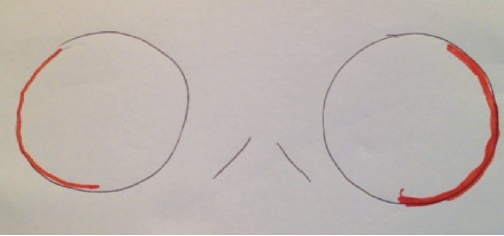
Figure 1. Sister A illustrated her experience of positive dysphotopsia.
Because of conflicting theories on the origin of positive dysphotopsia and how to resolve it in the literature, I decided to try two different approaches in early 2016 for both of Sister A’s eyes. Her emmetropic right eye underwent implantation of a Sulcoflex IOL (Rayner) with plano power. For her left eye, which had 0.50 D cylinder × 180°, I performed optic capture in front of the capsulotomy with a temporal approach. Both surgeries were uneventful.
One month after the second surgery, the patient’s symptoms had improved slightly, more so in the eye that had received the Sulcoflex IOL, but dysphotopsias persisted. UDVA was 0.06 and 0.00 logMAR and refraction was -0.50 +1.00 × 23° and -0.50 +0.50 × 10° in her right and left eyes, respectively. Notably, the sisters reported similar degrees of positive dysphotopsia, even though only the elder had undergone additional surgery. The younger sister was experiencing fewer disturbances, and she chose not to undergo further surgery to decrease dysphotopsias at that time.
Taking into account the persistence of the positive dysphotopsia, I offered to exchange the implanted IOLs for monofocal IOLs in both sisters at no charge. To my surprise, they both immediately refused my offer. They appreciated their unaided vision despite the photic symptoms, and they believed that the intensity of their symptoms was decreasing.
They both returned in 2017 and 2018 for follow-up visits, and they hardly mentioned the arcs of light during the latest visit, which lasted only 10 minutes compared with the 30- to 40-minute duration of earlier visits.
DISCUSSION
Out of the more than 200 patients in whom I have implanted the Pod FT IOL, these two sisters are the only ones who have reported experiencing positive dysphotopsia. When looking for the possible causes, I obtained corneal tomography after surgery, which showed a temporally displaced corneal apex with nasal fixation typical of hyperopia (Figures 2 and 3). Thus, a preoperative evaluation of corneal tomography (and not only of the anterior topography) would probably have anticipated these photic symptoms.
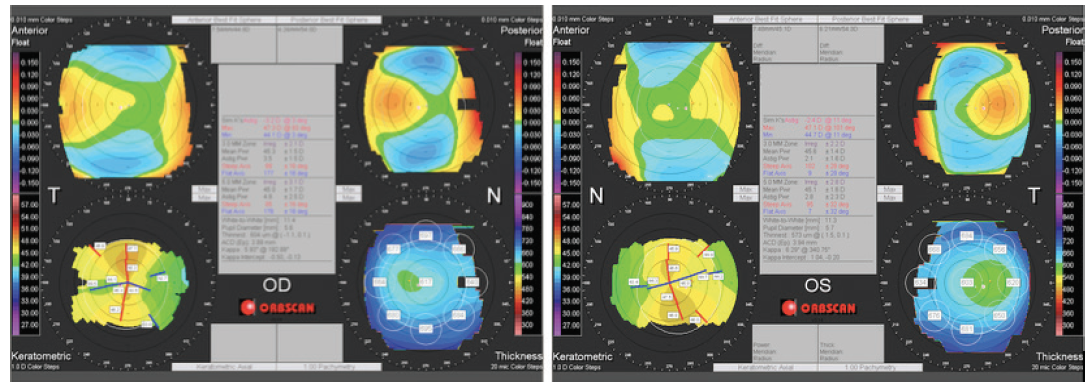
Figure 2. The postoperative corneal tomography of Sister A, who experienced more prominent symptoms.
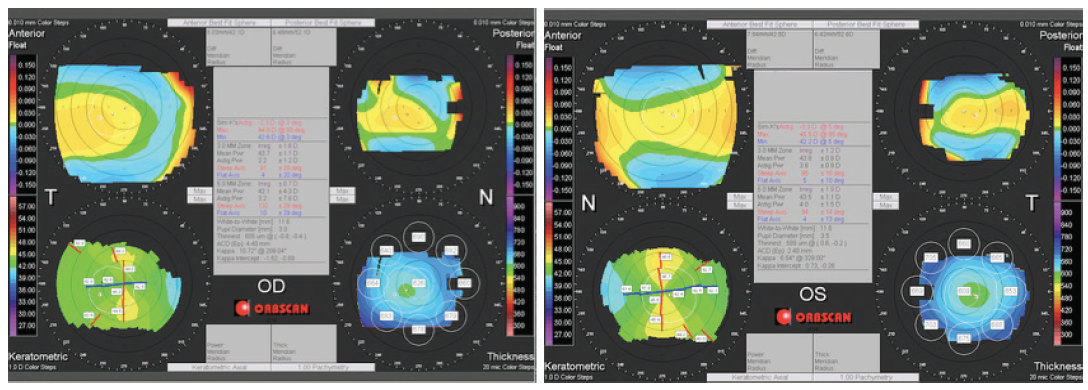
Figure 3. The postoperative corneal tomography of Sister B, who experienced less prominent symptoms.
Interestingly, the corneas of Sister B (the patient with fewer complaints) showed fewer abnormalities. The corneal irregularity and the decentration of fixation were identified as the causes of the dysphotopsia, making these two sisters poor candidates for multifocal IOL implantation. Given the tomographic corneal irregularities, I can understand why further surgery did not relieve Sister A’s symptoms. Additionally, I believe that even nasal decentration of the IOLs at implantation, if possible, would have yielded no better results.
Luckily, the advantages of spectacle freedom were so great that both patients eventually accepted the inconveniences instead of requesting IOL exchange. What I learned from this experience is to perform corneal tomography on every candidate for multifocal IOL implantation and to discuss the possibility of postoperative positive dysphotopsia, especially with high hyperopes. Further, it is important to remember that photic symptoms associated with multifocal IOL implantation tend to decrease over time, as evidenced in these cases.
