





Cataract surgery provides perhaps the best opportunity of any ophthalmic surgery to deliver an excellent refractive outcome for a patient. A refractive cataract procedure is distinguished from a typical cataract procedure because it involves active and conscious planning to deliver an increased quality of vision to the patient postoperatively. This will reduce the patient’s dependence on corrective lenses and, ultimately, drive patient satisfaction.
The refractive plan should be comprehensive and individualized for each eye of each patient, considering anatomic factors and optical properties along with the patient’s desires and expectations. Screening to identify patients at higher risk for complications and poor outcomes is a vital part of the preoperative assessment and a major concern for the refractive cataract surgeon.
CAREFUL SCREENING
As Sun Tzu said in The Art of War: “If you know the enemy and know yourself, you need not to fear the result of a hundred battles. If you know yourself but not the enemy, for every victory gained you will also suffer a defeat. If you know neither the enemy nor yourself, you will succumb in every battle.”
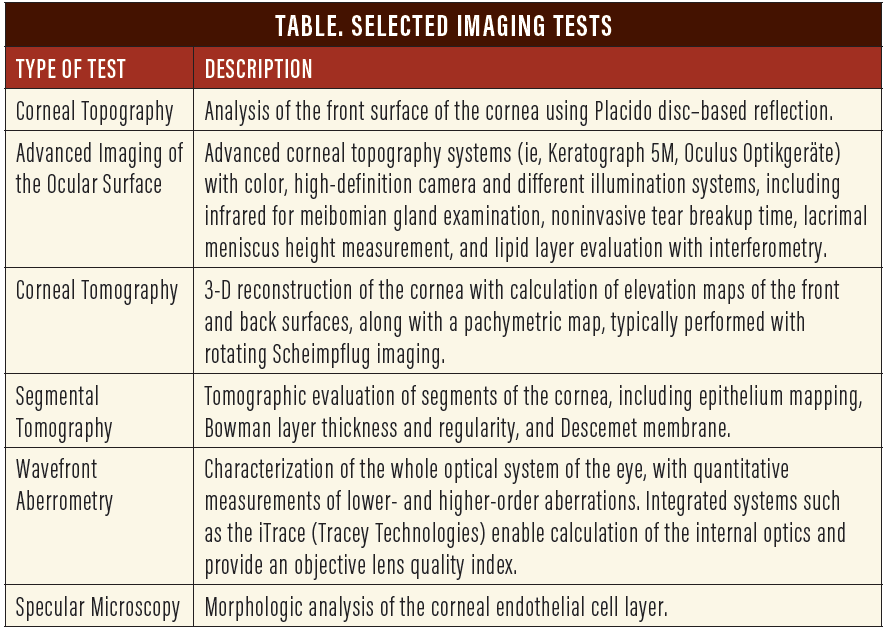
Thus, we should consider a similar strategy to prevent unhappy patients after any refractive procedure. We must understand the conditions to screen for preoperatively and know how best to apply our corneal and refractive imaging technologies for that purpose. The Table presents a sampling of imaging tests currently available.
The condition of the ocular surface, tear film status, and the optical regularity of the cornea (front and back) and its biomechanical properties and endothelial status are the most critical characteristics to be considered before surgery. We need to perform a comprehensive evaluation, considering both eyes together, including assessment of binocularity and enantiomorphism. Certain ocular biometrics (axial length, white-to-white distance, and lens thickness) are, of course, fundamental for IOL calculations. Also, vitreous transparency and the conditions of the optic nerve, macula, and peripheral retina are relevant for the best planning.
CONSIDERING THE OCULAR SURFACE
Safety and efficacy are key elements of refractive cataract surgery. Customized planning is required regarding many aspects of the procedure, including when best to do it, how to design the incision, and which IOL should be selected.
When choosing the IOL, the first consideration is the tear film. An irregular and unstable tear film will affect the biometric measurements for IOL power calculation. Likewise, after surgery, a poor tear film can degrade the quality of vision. In the Prospective Health Assessment of Cataract Patients’ Ocular Surface (PHACO) study, Trattler et al found that the incidence of dry eye disease in patients scheduled for cataract surgery was higher than previously thought; more than 50% of patients had a tear breakup time (TBUT) of 5 seconds or less, more than 75% of eyes had positive corneal staining, and 50% of eyes had positive central corneal staining.1
Because of the potential consequences for patients’ vision postoperatively, the need for ocular surface optimization must be identified and addressed before surgery. Figure 1 shows the meibography of a 65-year-old cataract patient with noninvasive TBUT of less than 7 seconds. Omega-3 essential fatty acid oral supplementation, preservative-free lubricants, and intense pulsed light therapy were indicated for this patient before measurements were performed for IOL calculation and planning.
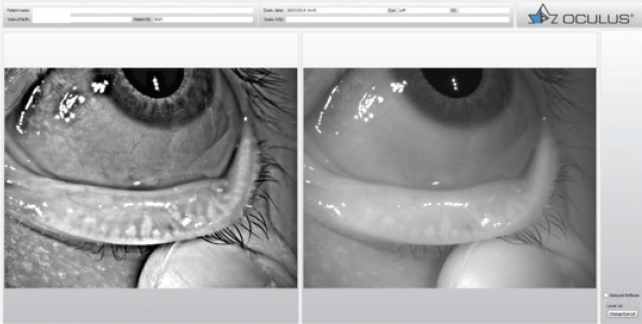
Figure 1. Meibography with the Keratograph 5M.
KERATECTASIA
The cornea’s optical status and structure must also be considered. This is important for determining, for example, whether the patient is a good candidate for a multifocal IOL, but also because the corneal status will help identify whether there might be a need for a corneal refractive enhancement after surgery. Progressive keratectasia after laser vision correction has emerged as one of the main concerns for refractive surgeons.2
Furthermore, there has been an increase in the prevalence of mild ectasia in cataract patients older than 65 years.3 This is particularly relevant in relatives of patients with keratoconus who remain undiagnosed until a detailed corneal imaging evaluation is performed,4 or those with mild, early, or forme fruste keratoconus that may be challenging to detect.5 Patients with even mild corneal ectasia have a greater chance of experiencing optical quality problems and postoperative dissatisfaction, especially with multifocal lens implants.5
Keratectasia screening has undergone a significant evolution in recent years.2 Placido disc–based corneal topography is an indispensable test for the evaluation of the corneal surface because it can help to detect ectasia before the loss of corrected distance visual acuity and the development of clinical signs at the slit lamp (Figure 2).5
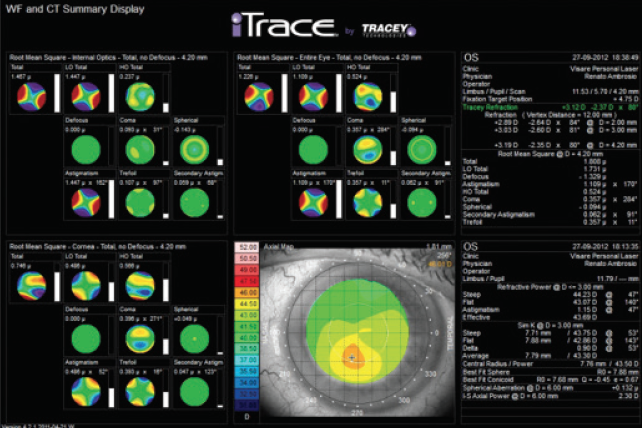
Figure 2. Placido disc–based corneal topography with iTrace, including corneal, ocular, and internal wavefront aberrometry of a 58-year-old patient with severe complaints after multifocal diffractive IOL implantation.
CORNEAL IMAGING TECHNOLOGY
In the past few decades, there has been a revolution in corneal imaging technologies, with the introduction of corneal tomography and methods of biomechanical assessment.6 Scheimpflug imaging–based corneal tomography allows 3-D reconstruction of corneal front and back surfaces and ray-tracing aberrometry of the entire cornea, giving valuable information on total corneal astigmatism and higher-order aberrations that can limit functional outcomes (Figure 3). The Belin-Ambrósio Deviation Index (BAD-D), available on the Pentacam (Oculus Optikgeräte), uses a regression model that combines the deviations of several parameters from normality to detect keratoconus with high sensitivity and specificity.5 The display provides standard and enhanced best-fit sphere elevation maps along with tomographic thickness profile data.7
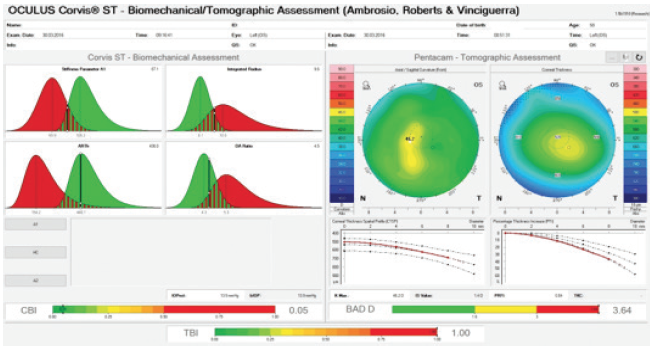
Figure 3. Integrated Scheimpflug biomechanical and tomographic evaluation from Corvis (Oculus Optikgeräte; left) and Pentacam (right). Note the tomographic biomechanical index score of 1, confirming mild keratoconus, which was not detected before surgery.
However, considering the possible need for corneal refractive enhancement after refractive cataract surgery, the identification of mild keratoconus is not enough. Our aim must be to address susceptibility to corneal ectasia.2 Lopes et al used artificial intelligence to develop the Pentacam Random Forest Index, with greater accuracy for detecting ectasia and susceptible cases than previous tomographic indices, including the BAD-D.8
More recently still, the Tomographic Biomechanical Index (TBI) was introduced as a combined parameter based on Scheimpflug-based corneal tomography and biomechanical assessments (Figure 3).6 Additionally, epithelial thickness mapping using segmental or layered tomography on OCT may provide additional information for detection of ectasia risk.9
Ocular aberrometry is another diagnostic tool that offers useful information about the refractive status of the eye. Irregular astigmatism resulting from corneal distortion is associated with a decrease in the optical quality of the cornea and an increase in lower- and higher-order aberrations.7
The characterization of the cornea preoperatively should also include an evaluation of the endothelium. The onset of corneal edema in Fuchs endothelial corneal dystrophy begins early in the course of the disease, resulting in a gradual increase in corneal thickness and corneal structural abnormalities.10
CONCLUSION
Planning for refractive cataract surgery requires an understanding of the diagnostic technologies available to aid in selecting the best IOL for each patient. The presence of corneal disease (eg, mild ectasia or endothelial guttae) is not necessarily an exclusion factor for refractive cataract surgery or an obstacle for a good refractive outcome, but it is a condition that implies the need for patient education and individualized planning.11
The ultimate goal of any refractive surgery is patient satisfaction with good quality vision. We advocate that every refractive cataract surgeon should be aware of this opportunity when planning any cataract procedure and should consider taking conscious advantage of the imaging armamentarium to optimize the chances of success and, ultimately, to make every cataract procedure a refractive one.
1. Trattler WB, Majmudar PA, Donnenfeld ED, et al. The prospective health assessment of cataract patients’ ocular surface (PHACO) study: the effect of dry eye. Clin Ophthalmol. 2017;11:1423-1430.
2. Ambrosio Jr R, Randleman JB. Screening for ectasia risk: what are we screening for and how should we screen for it? J Refract Surg. 2013;29(4):230-232.
3. Moshirfar M, Walker BD, Birdsong OC. Cataract surgery in eyes with keratoconus: a review of the current literature. Curr Opin Ophthalmol. 2018;29(1):75-80.
4. Karimian F, Aramesh S, Rabei HM, et al. Topographic evaluation of relatives of patients with keratoconus. Cornea. 2008;27(8):874-878.
5. Hallal Jr RJ, Ambrósio Jr R. The importance of screening for ectatic corneal disease prior to multifocal intraocular lens. International Journal of Keratoconus and Ectatic Corneal Diseases. In press.
6. Ambrosio Jr R, Lopes BT, Faria-Correia F, et al. Integration of Scheimpflug-based corneal tomography and biomechanical assessments for enhancing ectasia detection. J Refract Surg. 2017;33(7):434-443.
7. Salomão M, Hoffling-Lima AL, Lopes B, et al. Recent developments in keratoconus diagnosis. Exp Rev Ophthalmol. 2018;13(6):329-341.
8. Lopes BT, Ramos IC, Salomao MQ, et al. Enhanced tomographic assessment to detect corneal ectasia based on artificial intelligence. Am J Ophthalmol. 2018;195:223-232.
9. Belin MW, Ambrósio Jr R. Enhanced screening for ectasia risk prior to laser vision correction. International Journal of Keratoconus and Ectatic Corneal Diseases. 2017;6(1):23-33.
10. Sun SY, Wacker K, Baratz KH, Patel SV. Determining subclinical edema in Fuchs endothelial corneal dystrophy: revised classification using Scheimpflug tomography for preoperative assessment. Ophthalmology. 2019;126(2):195-204.
11. Montano M, Lopez-Dorantes KP, Ramirez-Miranda A, et al. Multifocal toric intraocular lens implantation for forme fruste and stable keratoconus. J Refract Surg. 2014;30(4):282-285.
