



I started correcting astigmatism 20 years ago, as soon as I completed my residency. At that time, I was taught limbal relaxing incisions, but I never fell in love with them due to their low accuracy. In 2011, I implanted my first toric IOL, and I then immediately stopped performing relaxing incisions and began my series of studies of astigmatism correction with Kristian Næser, MD.1-7
Today, about 50% of my patients receive toric IOLs, and about 65% of my multifocal IOL patients receive toric multifocal IOLs.
I believe that two steps should be followed to maximize the results of toric IOL implantation: First, surgeons must know the devices available in their clinic and be familiar with their measurements, and second, surgeons must learn vectorial calculations. Although the latter may seem challenging, vectorial calculations can help clinicians to better understand and refine the results of their surgery.
We routinely perform optical biometry using three devices: the Aladdin (Topcon), the OA-2000 (Tomey), and the Pentacam AXL (Oculus Opikgeräte). Formula constants are optimized for each of them. Usually, the results from the three biometers are very similar, and this increases our confidence in the predicted refraction.
For patients who are candidates for multifocal IOLs, we also take measurements by ultrasound immersion biometry and make our calculations again with optimized constants. This is important to confirm the results of optical biometry. If a discrepancy between optical and ultrasound biometry is observed, the patient is advised that there is a higher risk of refractive error.
For astigmatism, we measure total corneal astigmatism with the Pentacam AXL and with the Sirius (CSO). These measurements cannot be considered interchangeable, as previously demonstrated.5 Recently we have also begun measuring total corneal astigmatism with anterior segment OCT (MS-39, CSO) and total keratometry with the IOLMaster 700 (Carl Zeiss Meditec), but these values are used only for research purposes at this time.
I developed a formula with Dr. Næser, published in 2017, which optimizes keratometric astigmatism and, on average, provides the most accurate results in our experience.7 It is available on the website of the Italian Society of Ophthalmology (soiweb.com/toric-calculator/).
The calculator provides users with results in two sections: on the left, the optimized keratometric astigmatism (our formula), which is based on the measurements from the anterior corneal surface only; and on the right, the total corneal astigmatism based on Scheimpflug imaging (Figure). Having both methods is useful. If they provide similar results, I feel that the predicted refraction is reliable, and, if not, I perform more measurements (eg, using another Scheimpflug camera or anterior segment OCT).
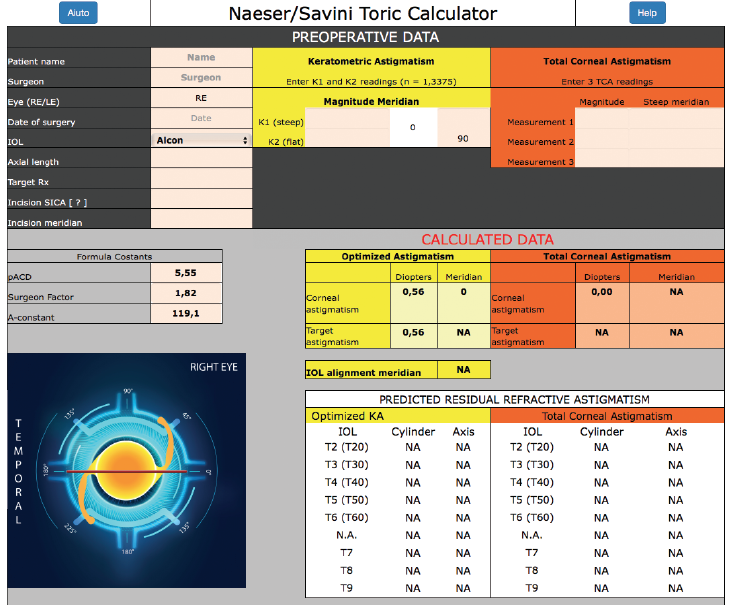
Figure. Screenshot of the online Næser/Savini Toric Calculator.
Find out what diagnostic devices I prefer in the Table here.
1. Savini G, Versaci F, Vestri G, Ducoli P, Næser K. Influence of posterior corneal astigmatism on total corneal astigmatism in eyes with moderate to high astigmatism. J Cataract Refract Surg. 2014;40:1645-1653.
2. Savini G, Næser K. An analysis of the factors influencing the residual refractive astigmatism after cataract surgery with toric intraocular lenses. Invest Ophthalmol Vis Sci. 2015;56:827-835.
3. Næser K, Savini G, Bregnhøj JF. Corneal powers measured with a rotating Scheimpflug camera. Br J Ophthalmol. 2016;100:1196-1200.
4. Savini G, Næser K, Schiano-Lomoriello D, Mularoni A. Influence of posterior corneal astigmatism on total corneal astigmatism in eyes with keratoconus. Cornea. 2016;35:1427-1433.
5. Savini G, Næser K, Schiano-Lomoriello D, Ducoli P. Total corneal astigmatism measurements: agreement between 2 rotating Scheimpflug cameras. Cornea. 2017;36:463-469.
6. Næser K, Savini G, Bregnhøj JF. Estimating total corneal astigmatism from anterior corneal data. Cornea. 2017;36:828-833.
7. Savini G, Næser K, Schiano-Lomoriello D, Ducoli P. Optimized keratometry and total corneal astigmatism for toric intraocular lens calculation. J Cataract Refract Surg. 2017;43:1140-1148.
