


I believe that refractive error is a disease of the eye—no different from glaucoma, dry eye disease, and other issues for which we readily offer treatment. In the world of modern cataract and refractive surgery, we have the capability to correct visual acuity that is compromised due to astigmatism and other types refractive error, so why shouldn't we treat astigmatism during cataract surgery?
A large percentage of our cataract patients, about 75%, have at least 0.50 D of astigmatism. Even this small amount of astigmatism can and often does create issues visually for patients. The higher the level of astigmatism, the more it can affect vision. My philosophy is, why not try to help these people? Correcting their astigmatism will help them to achieve better visual acuity, and this is even more crucial in patients who elect a multifocal, extended depth of focus, or other premium IOL.
It is important to educate patients about their astigmatism and to relay to them what we can do to correct it. The level of care and attention to detail affects everything, from our surgical outcomes, to the practice’s reputation, to future referral patterns.
THRESHOLDS AND BEST PRACTICES
My threshold for astigmatism treatment is about 0.75 D. Above that, the patient can lose contrast and can have functional visual acuity issues if the astigmatism is not addressed. I believe that correction of low astigmatism, especially, is low-hanging fruit, as it provides surgeons with an additional opportunity to improve their practices. We want to avoid patients experiencing loss of contrast sensitivity even though their cataract surgery was successful. By correcting that small amount of astigmatism, we can improve the outcomes for these patients—and happy patients refer other patients.
My other philosophical priority is to have available the proper treatment modalities to help patients achieve the best outcomes. We have a variety of tools to treat astigmatism. For low astigmatism, less than 1.00 D, I generally use manual or laser-assisted limbal relaxing incisions (LRIs). Although this can be a helpful strategy, the troubles with LRIs are that they are not consistent, they can close up, they can scar, and they can create nerve issues and, rarely, pain or a foreign body sensation. Additionally, LRIs are not predictable. They work when they work, but when they don't it is frustrating to both the patient and the surgeon.
It is for these reasons that I favor toric IOLs and use them in the vast majority of my patients who present with 1.00 D or more of cylinder. Today, with the availability of advanced technology IOLs, I can implant monofocal toric lenses even in patients with macular degeneration. I find that correcting the astigmatism really helps this population of patients; however, we take due diligence to set the proper expectations. We explain that these patients will not get to 20/20 postoperatively because they have degeneration.
The components of my preoperative workup are fairly standard. We make sure that the ocular surface is healthy and that the patient does not have chronic dry eye disease, which can interfere with topography or tomography readings. We use either Pentacam (Oculus Optikgeräte) or Cassini Total Corneal Astigmatism (Cassini Technologies) for corneal tomography measurement to ensure that we include the posterior astigmatism in our calculations (Figure). We also use the IOLMaster 700 (Carl Zeiss Meditec) or another biometry device, and we compare the results of all the machines to make sure they are consistent. If they are not, I have the patient return for rescanning. The best diagnostic tool for posterior segment issues is OCT of the macula and optic nerve, which can reveal membranes that did not appear on slit-lamp examination.
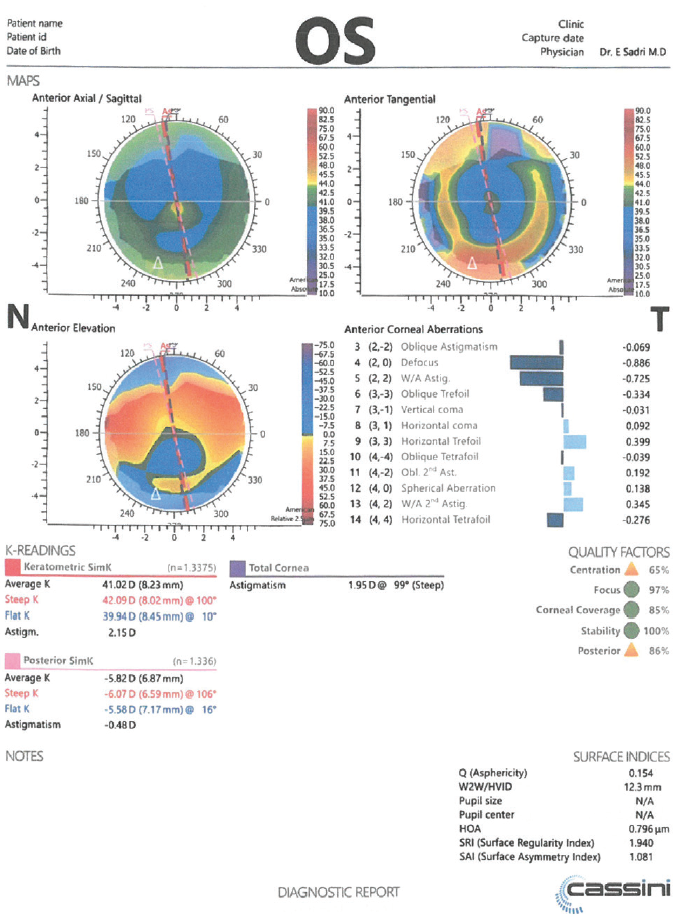
Figure. Total corneal astigmatism measurements from the Cassini.
CONCLUSION
Astigmatism correction is not a difficult task. With the right basic preoperative workup and with minimal additional tools, surgeons can safely and reliably measure astigmatism and plan the best approach for its correction during cataract surgery. In my hands, most of the time, that is a toric IOL.
I believe that, today, we must address astigmatism at the time of cataract surgery. When we do not, it is a disservice to our patients.
Find out my preferred diagnostic devices in the Table here.
