


The concept proposed in this article may come across as radical, but, when you consider my reasoning, I think that you can find some sense in its proposition. This article is based on a talk I gave in June at the American-European Congress of Ophthalmic Surgeons (AECOS) 2019 European Symposium in Sitges, Spain. It explores where I think refractive surgery fits into all of ophthalmology and explains how it differs from nonrefractive ophthalmology.
Some eye care practitioners regard refractive surgery as a side dish on the plate of ophthalmology. But consider the global statistics on visual impairment: The single biggest cause of visual impairment, at 43% of the global burden, is uncorrected refractive error. The second-leading cause, at 33%, is cataract.1 These two conditions are by far the greatest contributors to global visual impairment, and today both can be considered forms of refractive surgery.
Consider also the importance of vision in human functioning. The sensory input to the brain is predominantly visual; touch, hearing, and smell collectively make up less than 40% of all sensory input, whereas vision involves 60% of the brain.2 As for speed of data transmission within the brain, sight is transmitted 10 times faster than touch and 100 times faster than hearing or smell.2
Furthermore, of the millions of people worldwide who require spectacle correction, in many countries less than 25% of people who need them actually have spectacles, and in some parts of the world this number doesn’t go above 50%. When one takes into account the global cost of impaired vision to the individual, to the individual’s family, and to the local and the larger environment, the cost is enormous. Correcting visual errors with refractive surgery could completely transform the lives of millions of people. To correct even some portion of these refractive errors is, however, a huge task and one that requires tremendous effort.
DIFFERENCE OF REFRACTIVE SURGERY
Let’s explore how refractive surgery differs from nonrefractive, or disease-based, ophthalmology.
Difference No. 1. At present, ophthalmology is oriented toward treating and restoring the health of the eyes. Most of ophthalmology, in other words, is disease-based. Refractive surgery, by contrast, is performance-based. Individuals with good spectacle- or contact lens–corrected acuity opt to undergo a procedure so that they can do without optical aids.
In this scenario, the demands on the surgeon for an excellent result are higher than in disease-based surgery, and the knowledge and training that it takes to achieve excellent results on an ongoing basis is far beyond what is taught in medical school. This is one reason why refractive surgery is so different from disease-based medicine.
Difference No. 2. In order to perform refractive surgery at the highest level and with the highest safety, we are heavily dependent on technology. In turn, running a refractive clinic is more costly and challenging than most other ophthalmologic services. The surgeon now must also be an entrepreneur. This is another way in which refractive surgery is different from disease-based medicine.
Difference No. 3. At present, refractive surgery is mostly practiced as a self-pay enterprise; this again differs from disease-based medicine, which is generally reimbursed by private or public insurance. Working with patients who pay for their procedures themselves presents a higher level of patient expectation, and again another requirement for education for surgeons in this field.
Difference No. 4. The only acceptable outcome in refractive surgery is excellent (some would even say perfect) vision. The decision to undergo refractive surgery rests with the individual. For this reason, people usually pay for refractive surgery with their own money rather than through insurance. This is perhaps the most visible manifestation of the difference between refractive surgery and disease-based ophthalmology, and it is the one that often generates unfortunate resentment and mistrust among our nonrefractive colleagues.
COST SAVINGS AND PROFESSIONAL BENEFITS
For an individual in the developed world, undergoing refractive surgery has the potential to produce a lifetime cost savings of between €16,000 and €35,000 in comparison with glasses and contact lenses. We also know today that refractive surgery is safer than contact lens use3,4 and provides individuals with a better lifestyle, more convenience, and better occupational fitness.
It’s no surprise that first-line responders, police officers, professional athletes, and others who rely on their eyes for their professions opt for refractive surgery far sooner than others. It’s also important to note that refractive surgeons have undergone refractive surgery far more frequently than any other group of individuals on the planet—by a factor of five, to be exact.5
FORMAL TRAINING NEEDED
Given the global burden of uncorrected refractive error, we must train more eye care practitioners in refractive surgery so that we can adequately deal with current and future demands. At this time, refractive surgery is not taught during formal ophthalmology training, and most surgeons rely on short courses and peer-to-peer observation to try to hone their skills. Prior to the AECOS meeting in Sitges, I sent out a survey to registered delegates. The results I gathered indicated that the overwhelming majority of respondents to that questionnaire (more than 70%) were self-taught, and only a minority had formal training. When asked about future training requirements, more than 80% in the same group said they anticipate creation of a formal fellowship for refractive surgery.
If we want to deliver excellence on a global scale and on a repeatable basis, we must enhance the training of young surgeons so that all surgeons are fully competent in refractive surgery with negligible complication rates. And, paramount, they must know how to manage complications.
In the 1930s, plastic and cosmetic surgery separated from reconstructive surgery with the formation of the American Board of Plastic Surgery (ABPS; https://www.abplasticsurgery.org/). The ABPS was given the status of a major medical specialty in the 1940s, and today approximately 7,000 active surgeons have ABPS certification. General surgeons, otolaryngologists, ophthalmologists, and other practitioners may not be members of ABPS but may still perform plastic or cosmetic surgical procedures in a competent fashion.
To enable the public to confidently access practitioners with a prescribed level of knowledge transfer, skills transfer, skills performance, clinical skill maintenance, and ethical practice, it is helpful for surgeons to be part of a large organization such as the ABPS. The board’s mission is to promote safe, ethical, efficacious plastic surgery to the public by maintaining high standards for the education, examination, certification, and continuous certification of plastic surgeons as specialists and subspecialists.
The parallels between plastic and, especially, cosmetic surgery and refractive surgery are striking. Refractive surgery is different from general ophthalmology in a number of ways, as previously outlined in this article. Our training must reflect this difference so that, once refractive surgeons enter practice, they are equipped to deal with the increased level of public scrutiny (more so than in any other area of eye care), increased patient demands, and increased requirements of understanding and using technology.
Now may be a good time to initiate such formal training, with increasing awareness of the impact of uncorrected refractive error on the global economy and the wellbeing of the planet’s citizens. Given this awareness, the lack of a plan to train refractive surgeons for the future is notable. My son has just commenced year 4 of a 7-year training program in ophthalmic surgery that is widely regarded as an excellent training experience. I can safely predict that, during these 7 years, he will witness not one LASIK or SMILE procedure, not one phakic IOL implantation, not one toric or multifocal IOL implantation, and certainly no surgical procedure for presbyopia. What is to be done about this situation?
FUNCTION VERSUS PATHOLOGY
Refractive surgery relies on excellent ophthalmic skills for clinical and surgical management. In that respect, our general ophthalmic experience provides the foundation for refractive surgery. However, refractive surgery is fundamentally different from ophthalmology in that its focus is on function rather than pathology.
Like plastic surgery, refractive surgery relies on a foundational skill set that is applied to advance performance, lifestyle, and appearance. This may explain why many of our nonrefractive ophthalmology colleagues view refractive surgeons as foreign. Combating pathology is a fight against loss; refractive surgery is a pursuit of gain.
Valuing loss over gain permeates much of humanity’s outlook, even beyond our profession—particularly in the field of economics. This has been demonstrated in behavioral economics and psychological experiments. Kahneman and Tversky in 1979 described what they called the prospect theory, positing that people will prioritize avoiding small losses over seeking larger gains.6 This is part of human nature.
A primary goal of disease-based ophthalmology is to avoid loss—to stop the decline of cataract blindness, slow glaucoma, prevent diabetic retinopathy—and this leads to admirable and important results. The focus on loss supports a framework of insurance to share risk. It promotes the view that conservative therapy means minimizing risk, rather than striving for potential improvement.
The context of refractive surgery, and of those who work in the field, is fundamentally different. The goal—improving performance, lifestyle, and personal appearance—requires striving for gain. This sets a high bar for performance at every level, including in training; technical skills; familiarity with technology; patient selection; surgical care; and, yes, business, culture, marketing, and research.
A COLLEGE OF REFRACTIVE SURGERY
Improving patients’ quality of life is a worthy pursuit. Refractive surgery can improve quality of life for patients in every waking minute of their days. Benefits are seen in lifestyle, convenience, occupational fitness, personal economics, safety, and appearance. We create value as we pursue gain.
The Refractive Surgery Alliance (RSA), of which I am a member, has defined the initial leadership, structure, and goals for a proposed College of Refractive Surgery, and we look forward to your active participation. The College of Refractive Surgery will define a new approach. Its focus will include education, accreditation, and impact assessment, and its reach will be expansive.
The College of Refractive Surgery will provide the curriculum and oversight, and the RSA’s network of refractive surgeons will provide the training and mentoring. Work is under way by RSA members in different parts of the world to identify where the greatest burden of need is.
We look forward to seeing everybody win. The visually impaired can be made to see; trainee refractive surgeons can be taught by masters in their environments and then apply the surgical skills hands-on in hundreds of cases; and refractive surgery can be elevated to where it belongs: a modern miracle of science, technology, safety, and efficacy that has the potential to change the world for the better. If we do not do this now and start to rid the world of this congenital defect, when will we ever do it?
1. World Health Organization. Global data on visual impairment. https://www.who.int/blindness/publications/globaldata/en/. Accessed July 15, 2019.
2. Nørretranders T. The User Illusion: Cutting Consciousness Down to Size. New York; Penguin Press Science; 1999.
3. Masters J, Kocak M, Waite A. Risk for microbial keratitis: Comparative metaanalysis of contact lens wearers and post-laser in situ keratomileusis patients. J Cataract Refract Surg. 2017;43(10):67-73.
4. Price MO, Price DA, Bucci FA Jr, Durrie DS, Bond WI, Price FW Jr.
Three-year longitudinal survey comparing visual satisfaction with LASIK and contact lenses. Ophthalmology. 2016;123(8):1659-1666.
5. Kezirian GM, Parkhurst DG, Brinton JP, et al. Prevalence of laser vision correction in ophthalmologists who perform refractive surgery. J Cataract Refract Surg. 2015;41:1826-1832.
6. Kahneman D, Tversky A. Prospect theory: an analysis of decision under risk. Econometrica. 1979;47(2):263-292.
Corneal refractive surgery should not be its own specialty for the same reason that cataract surgery is not one: because it is so fundamental to clinical practice that all ophthalmologists should learn it during residency.
I’ve been performing corneal refractive surgery since 1989, when I participated in some of the first US excimer laser clinical trials. After PRK was approved by the US FDA in 1996, my colleagues and I at the University of Louisville acquired an excimer laser, and we’ve effectively been operating a laser center much like a timeshare ever since, with more than 25,000 refractive surgeries performed there to date. Of our 25 owner-users, only two of us are cornea specialists. The rest are cataract surgeons or general ophthalmologists who are more than capable of performing corneal refractive surgery safely and effectively.
Because of this long experience and our close association with the university (although the laser center is privately owned), we have made a commitment to teach residents at the University of Louisville how to perform PRK, LASIK, and phototherapeutic keratectomy as part of their residency training through a partnership with Johnson & Johnson Vision. All participants receive didactic training and wet-lab training with pig eyes, and those who wish to become certified perform 10 cases under supervision. This year, we expect all of our senior residents and half of the junior residents to become certified (Figure 1).
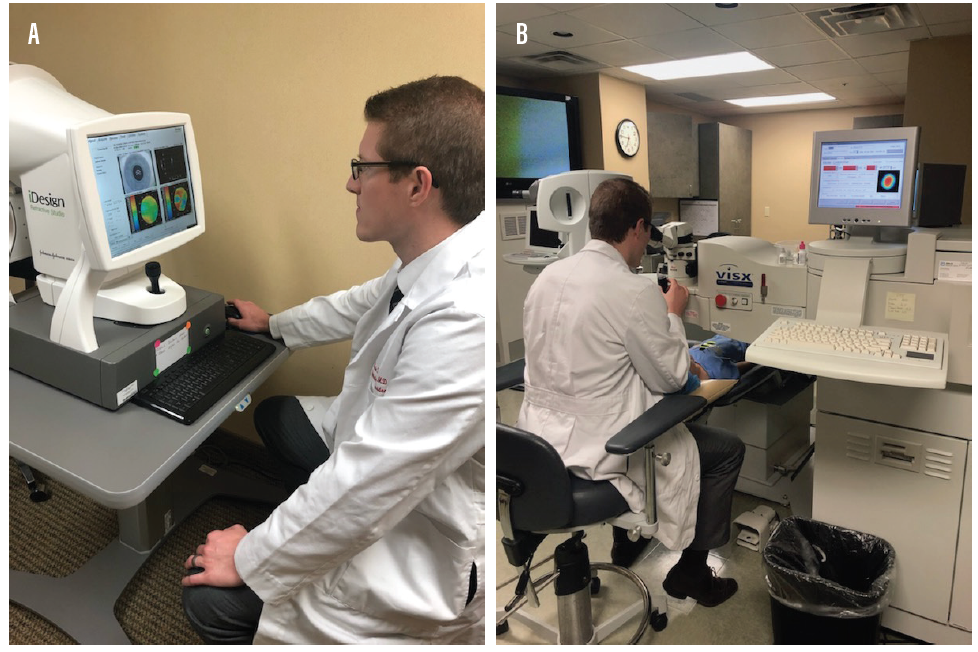
Figure 1. Second-year resident Kevin Lowder, MD, plans a wavefront-guided ablation (A) and performs an LVC procedure (B).
Figures 1 and 2 courtesy of Richard A. Eiferman, MD
Refractive surgery is no different from other surgical procedures we routinely teach residents. Surgeons in training learn to perform phacoemulsification and IOL implantation (by far the largest component of their training), muscle surgery, glaucoma surgery, corneal surgery, and retina surgery. Patients at teaching centers accept that the benefits of being treated at a teaching center—access to world-renowned experts, cutting-edge research and clinical trials, and relatively high rates of charity care—also mean that all or part of their surgery may be performed by a resident under the supervision of an experienced surgeon. In many cases, including refractive surgery, that means patients get free or less expensive care that they might otherwise be unable to afford.
RESIDENTS WANT EXPOSURE
In a survey conducted by the ASCRS, more than 60% of young ophthalmologist respondents reported that they felt their laser vision correction (LVC) experience during residency had been inadequate.1 The authors of the study concluded that young ophthalmologists lack experience in refractive surgery and new IOL technologies, not only in residency but even during their first 5 years in practice.
In my opinion, ophthalmologists do not need a full year of specialty fellowship training to become proficient in corneal refractive surgery, they simply need access to the technology and good to mentors. Nehls et al found that patients whose laser refractive surgery was performed by residents and fellows had high levels of satisfaction, improvement in refractive error, and improvement in quality of life 1 year after surgery.2 Published studies have also validated the safety and efficacy of refractive surgery performed by surgeons in training.3,4 In one of these studies, researchers at Walter Reed Army Medical Center found no statistically significant differences in outcomes between procedures performed by residents and those performed by staff surgeons.3
In an unpublished analysis of results obtained by our residents at the University of Louisville, the postoperative outcomes were excellent (Figure 2). At patients’ last follow-up appointments, 97% of PRK eyes and 85% of LASIK eyes were 20/20 or better and 55% and 32%, respectively, were 20/15 or better.
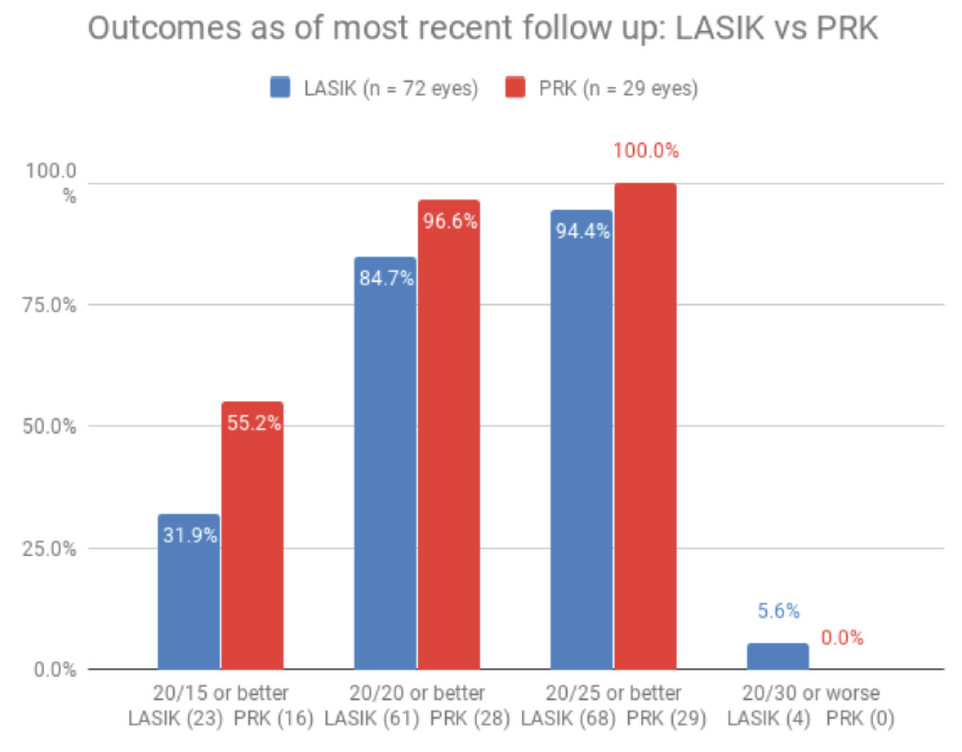
Figure 2. In 101 eyes treated by residents at the University of Louisville in 2018 and 2019, most achieved a UCVA of 20/20 or better postoperatively.
REFRACTIVE CATARACT SURGERY
Historically, if he or she preferred, a cataract surgeon could enjoy a successful career without knowing much about corneal refractive surgery. With the advent of refractive cataract surgery, advanced-technology IOLs, and elevated patient expectations for visual results after surgery, however, LVC now belongs in the armamentarium of every ophthalmologist who performs cataract surgery.
With contemporary refractive cataract surgery, it is important for surgeons to be able to address small amounts of residual refractive error, either sphere or cylinder, postoperatively. Those who can’t perform LVC in-house are at a significant financial and competitive disadvantage and may not be able to achieve the outcomes their patients expect.
Learning PRK and LASIK teaches young ophthalmologists a number of important skills that cross over into other areas of practice. Some of these are clinical, and others are more philosophical. On the clinical side, for example, the ability to read topographic and wavefront imaging gives residents greater insight into optics and ocular physics. Seeing the flattening or steepening of specific areas of the cornea helps them to grasp complicated concepts such as astigmatic meridians and higher-order aberrations. Learning to dock a femtosecond laser will make the learning curve shorter in the future, regardless of which cataract or refractive lasers they might use in practice.
Learning refractive surgery also helps our residents master some of the softer skills of ophthalmology, such as how to be conservative and cautious in looking for preoperative risk factors, how to talk to patients about private-pay procedures, and how to say no to poor candidates.
LVC CERTIFICATION
I believe that it is our job as educators to prepare students with the skills they need for clinical practice—including corneal refractive surgery. Many young ophthalmologists today enter practice with significant debt from undergraduate and medical school, so the sooner they can become productive, revenue-producing surgeons, the better.
Without refractive surgery training in residency, it can be hard to obtain certification later in practice. It may be difficult to convince a local competitor to teach a young surgeon the basics of refractive surgery and proctor his or her first cases, for example.
Being certified to perform corneal refractive surgery makes our graduates more marketable. LVC is a valuable skill set they bring to the practices that hire them, and it is one they can immediately use to build a patient base or to provide a service that other cataract surgeons in the practice might lack. Will freshly minted ophthalmologists be fabulous cataract surgeons on day 1 in practice? Of course not. But if they can do all of the practice’s refractive surgery, without referring those cases out, they can add value to the practice from that very first day.
Although few ophthalmology programs currently offer corneal refractive surgery training during residency, it is my hope that more will begin to do so. Refractive surgery can and should be integrated into the ophthalmic residency program, but it shouldn’t be considered its own specialty.
1. Schallhorn JM, Ciralsky JB, Yeu E. Resident and young physician experience with complex cataract surgery and new cataract and refractive technology: Results of the ASCRS 2016 Young Eye Surgeons Survey. J Cataract Refract Surg. 2017;43(5):687-694.
2. Nehls SM, Ghoghawala SY, Hwang FS, Azari AA. Patient satisfaction and clinical outcomes with laser refractive surgery performed by surgeons in training. J Cataract Refract Surg. 2014;40(7):1131-1138.
3. Weber ML, Stutzman RD, Mines MJ, et al. Residency training in refractive surgery. J Cataract Refract Surg. 2012;38(11):1962-1969.
4. Wagoner MD, Wickard JC, Wandling GR Jr, et al. Initial resident refractive surgical experience: outcomes of PRK and LASIK for myopia. J Refract Surg. 2011;27(3):181-188.
Refractive surgery has come a long way since the days of Professor José Ignacio Barraquer’s keratomileusis and keratophakia procedures that launched the era of modern surgical vision correction.1 Today, we have access to a wide range of surgical approaches and devices to correct myopia, hyperopia, and astigmatism with startlingly high success rates, and we have increasingly good approaches to treat presbyopia as well. Equally startling is the low penetration of refractive surgery among the population of potential candidates. For example, 42% of the US population has clinically important refractive error amenable to laser vision correction, but only 13% of that population has been treated.2
With so many possible ways to approach the problem of refractive error, it’s a daunting task for a surgeon to be sufficiently expert to bring the right tool to bear for every patient. Every cataract surgeon is a potential refractive surgeon, at least within the domain of refractive cataract surgery. But even looking at routine cataract surgery, there are 100 or more key considerations toward achieving the best results that aren’t taught in most residencies.
Some residents aren’t even exposed to the sorts of questions they should be asking to learn refractive cataract surgery. Many programs focus on simply getting the cataract out, which is the bare beginning of the procedure. Further, cataract surgery, and its close relative refractive lens exchange, are just one piece of the puzzle. Of any refractive surgical procedure, cataract surgery is the one best addressed during residency, and even that training still leaves much to be desired.
CORNEA FELLOWSHIP?
So if residency doesn’t provide mastery of the myriad ways to perform refractive surgery, where does that training happen? Many but not all refractive surgeons have a cornea fellowship background, and certainly such a fellowship can provide useful skills and knowledge. On the other hand, a comprehensive ophthalmologist with the right mindset to explore, learn, and seek appropriate mentors could gain a more thorough training in refractive surgery than many cornea-trained doctors receive.
This isn’t to say that cornea fellowships aren’t valuable, but rather that the skills and knowledge transferred through them vary wildly. Some fellowships focus almost exclusively on pathology, others on refractive surgery, and many on a variable mix of the two. There is no formal coursework in refractive surgery—no prescribed set of skills and knowledge that must be mastered to declare a graduate ready to be a refractive surgeon. A cornea-trained LASIK surgeon operating for the first time outside of fellowship might have treated 0, 10, 50, or hundreds of eyes to date.
PUBLIC CONFIDENCE
This variability matters for surgeons who desire expertise, of course (although these individuals may not even know what they do not know), but it may matter even more to the public. Public confidence will be vital if we are to achieve growth of refractive surgery into double-digit percent penetration and onward, to the point at which refractive surgery is often chosen instead of contact lenses or glasses, which have their own substantial risks and inconveniences. Formalized education in the domain of refractive surgery, with an associated certification, would be a great contribution in this direction.
There are significant reasons for ophthalmologists, young and old, to support the formation of a college of refractive surgery that would provide the necessary curriculum and backing for a specialization in this field. Existing cornea fellowship programs that already cover these procedures well and provide sufficient exposure to fellows could rebrand immediately as cornea and refractive surgery fellowships, whereas others that do not focus on this area would be understood to have a different focus.
The newly formed college would have to consider carefully how best to bring existing surgeons into the fold, perhaps via a combination of peer review and formalized testing. Many details of implementation must be fleshed out, but I think the need for our community and benefit to our patients is clear. It is time to implement a college of refractive surgery.
1. Barraquer JI. Queratoplastia refractive. Estudios Inform. 1949;10:221.
2. Kezirian GM, Parkhurst GD, Brinton JP, Norden RA. Prevalence of laser vision correction in ophthalmologists who perform refractive surgery. J Cataract Refract Surg. 2015;41(9):1826-1832.
If you look up medical specialty online, you’ll find a definition similar to the following: “a branch of medical practice focused on a defined group of patients, diseases, skills, or philosophy.”
Study that definition closely, as it embodies everything we are as physicians and ophthalmologists. It also distinctly embodies the history, practice, skill set, culture, and values of refractive surgeons.
Inclusion of the word philosophy in the definition of medical specialty may surprise you, but I didn’t put it there—Galen, first century Greek physician and founder of empirical thinking in medicine, did. He regarded medicine as an interdisciplinary field that was best practiced with theory, observation, and experimentation in conjunction with active learning in the physical practice of medical care. He considered the best physicians to also be philosophers. Even in Galen’s time, more than 2,000 years ago, our field was recognized as interdisciplinary, encompassing separate specialties with separate philosophies of medical and surgical care. The restoration of the physiologic functions of the human being has been the goal and the raison d’être of medicine and surgery for any practitioner of the art for several millennia.
The philosophy of refractive surgery, in accordance with Galen’s principle, is the restoration of visual function to ametropes without the aid of traditional prosthetics (ie, glasses and contact lenses). Wearing glasses or contacts continues to represent a handicap and even a risk in the performance of normal daily functions. This is the all-encompassing template driving every innovation in refractive surgery for the past century.
TECHNOLOGICAL ADVANCES
From this mandate has arisen the need for refractive surgeons to develop different surgical skill sets, including astigmatic keratotomy, radial keratotomy, conductive keratoplasty, PRK, LASIK, IOL (presbyopia-correcting and toric) implantation, phakic IOL implantation, laser cataract surgery, SMILE, corneal inlay implantation, and CXL.
Refractive surgery has led the way in our field’s technological advances. Optical biometry, advanced IOL power calculations, ultrasound, topography, intraoperative aberrometry, optical quality analyzers, and corneal analyzers are just a handful of examples. The engineers and scientists responsible for these and other technological marvels have helped us to identify the data and automate the procedures that are refining and defining the future of vision correction.
A NEW TYPE OF PATIENT, A NEW TYPE OF PRACTICE
Our society has reached the moment of critical mass when sociological, societal, psychological, and technological changes are causing a profound shift in human behavior. Today, freedom of vision without the aid of prosthetic devices is considered by many to be a basic right, and millions of patients have already experienced the joy and benefits of refractive surgery.
Practice patterns in refractive surgery have evolved to accommodate the internet’s digital disruption. Information culture and virtual reality have produced a new kind of patient-consumer—one who is service-oriented and whose visual goals approach perfection—and they have replaced the roles of traditional medical practices, institutions, and value systems. This combination has driven refractive surgeons and their practices to become highly skilled at marketing, offering cash-pay initiatives, enhancing the patient experience, fine-tuning patient consultations and counseling, mastering surgical skill sets, and incorporating the necessary technology.
THE IMPACT OF PHYSICIAN EDUCATION
Physician education in refractive surgery is a massive undertaking. Professional societies such as the AAO, ASCRS, AECOS, Society for Excellence in Eyecare, RSA, and many others offer a dazzling array of educational opportunities to master the field of refractive surgery.
Refractive surgery requires more than book learning, and much of the knowledge needed is not adequately covered in current residency programs. Refractive surgery is a major, immersive, mentored, continuing medical education discipline that, in my opinion, requires a physician commitment that has no equal in 21st-century medicine.
A PLEA FOR THE REFRACTIVE SURGERY SPECIALTY
Remember the definition of medical specialty from my opening paragraph—“a branch of medical practice focused on a defined group of patients, diseases, skills, or philosophy”? Refractive surgery meets and exceeds these requirements. In 1916, ophthalmology was the first branch of medicine to offer specialty board certification, now a standard among medical specialties. Yet the American Board of Medical Specialties (ABMS) does not recognize any specialties or subspecialties in ophthalmology because the organization was concerned about the adequacy of training and the level of qualifications required in ophthalmology.
Formed in 1933, the ABMS recognizes 24 specialty medical boards, the last of which was established in 1991. Over the past 86 years, more than 149 specialties and subspecialties have been formed across these 24 boards, most of which fall under the umbrellas of internal medicine and pediatrics at 20 apiece. It is stunning that ophthalmology had the first medical specialty board but is one of only five ABMS boards with no recognized specialties or subspecialties.
This field is way beyond compelling arguments and erudite discourse on the judgement of the value of refractive surgeons to patient care. The adequacy of training and the level of qualifications required to become a refractive surgeon are clear. After 103 years, it is time that we demand that refractive surgery be recognized as a separate medical specialty. Vision for life!
