

My routine cataract procedure today is laser cataract surgery. In this article, I will make reference to an accompanying Eyetube video that demonstrates my technique (bit.ly/haefliger0220).
I administer intraoperative antibiotics in all cases. My regimen is gentamycin 80 mg/2 mL (Hexal) 1 mL in 500 mL balanced saline solution. I use the Catalys Precision Laser System (Johnson & Johnson Vision) to create a capsulotomy and a six-sided fragmentation pattern. After the laser portion is complete, I make the paracenteses with a ClearCut HP2 2.4-mm diamond blade slit knife or a V-Lance 20-gauge knife (both by Alcon) through the conjunctiva rather than through clear cornea (Figure 1). I prefer to use this location for the incisions in order to avoid interfering with the refractive portions of the cornea and to reduce the risk of infection. After injecting irrigating fluid through a paracentesis, I fill the anterior chamber with Viscoat or ProVisc (both by Alcon).
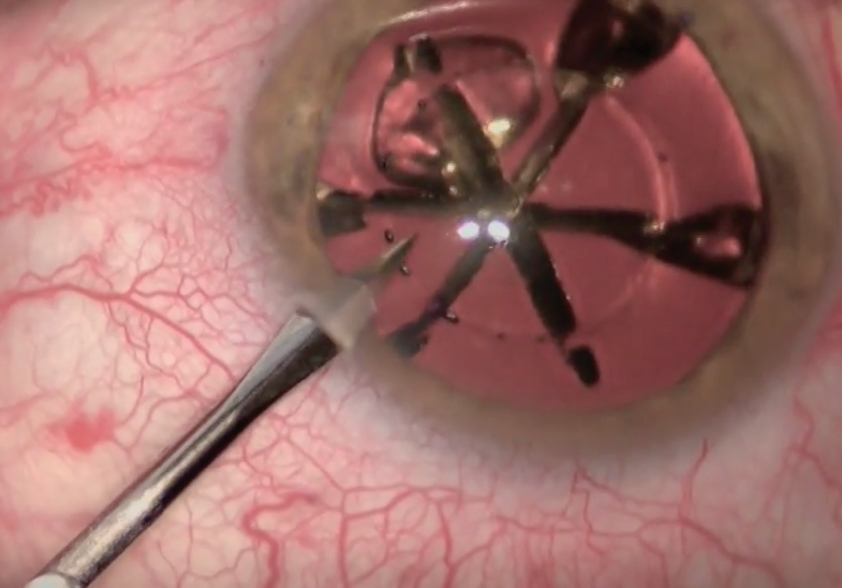
Figure 1. A paracentesis is made in the conjunctiva rather than the clear cornea.
I outline the 2.2-mm main incision with the pointed paracentesis knife and then complete it with a keratome, again through the conjunctiva rather than clear cornea. There may be some blood, but the antibiotic regimen will guard against infection. Once the incision is completed, I use the forceps to remove the free-floating capsulotomy created by the laser.
NUCLEUS REMOVAL
Hydrodissection is not always necessary with laser cataract surgery, as the air bubbles created by the laser separate the tissues well enough in some cases. After the nucleus is mobilized, I can begin separating and emulsifying the six nucleus segments that were created by laser fragmentation.
The second instrument you will see me using in my left hand is the Haefliger Femto Spoon (Geuder), which I developed. Even through a small paracentesis, this relatively large spoon can be inserted easily. I use a bimanual technique with the spoon and the phaco tip, separating the six segments from each other, rotating them toward the phaco tip of the OS 4 (Oertli Instrumente), and emulsifying them one by one (Figure 2).
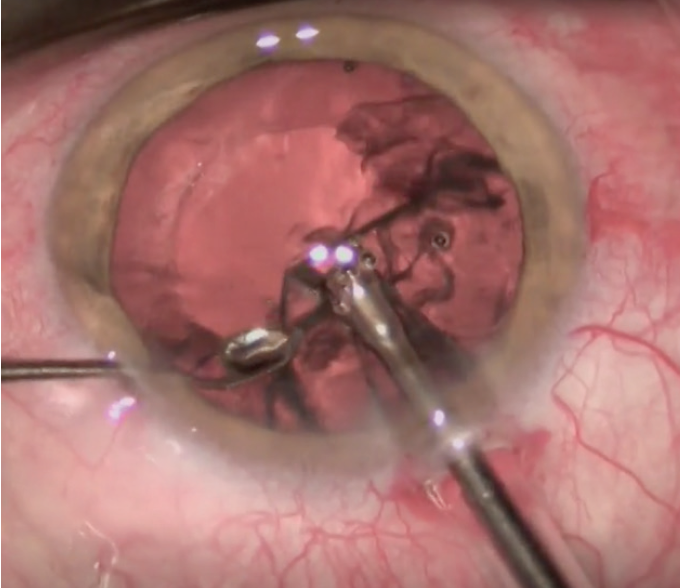
Figure 2. The Haefliger Femto Spoon is used to separate and rotate the six segments.
Many of the lens procedures I perform are refractive lens exchanges (RLEs). Often, these soft, clear lenses can be separated to the periphery using the large flat surface of the spoon. The device does not sink into the lens matter of a soft nucleus. It is important to separate the pieces out to the periphery in order to perform controlled evacuation in the center, in the deepest part away from dangerous areas in the lower periphery.
IRRIGATION AND ASPIRATION
I perform bimanual irrigation and aspiration with tips that I designed in 1990 (Bimanual Irrigation Aspiration System, H.P. Braem). What I call the nose of the airplane of the aspiration tip easily fits through a small paracentesis. The radius of curvature of the instrument gets smaller toward its tip, increasing the pressure per surface area and allowing it to gain easy access through the small paracentesis.
I prefer to implant the IOL under an OVD, mainly because, as I noted, many of these surgeries are RLEs, and safety is paramount. There is seldom a problem even when we perform lens implantation under balanced saline solution alone, but no risk is taken in these cases.
IOL INSERTION
Alignment of the axis of the toric lens I am implanting in the video (AcrySof IQ SN6AT4, Alcon) is established according to reference points made on the cornea. I use a curved 27-gauge hydrodissection cannula (Luftkanüle Modell Frankfurt, Geuder) to tweak the orientation of the IOL (Figure 3). I identify a landmark that allows me to judge and determine the right axis. Our outcomes analysis tells me that the average implant is less than 2° off its intended axis postoperatively.
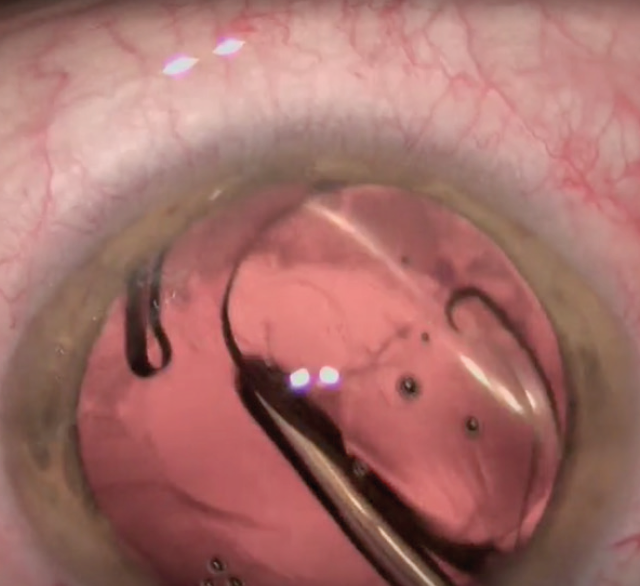
Figure 3. A curved hydrodissection cannula is used to tweak the orientation of the IOL.
Once the IOL is in place and well centered, with the capsulotomy overlapping the optic edge 360º, the lips of the conjunctiva are coapted to improve the postoperative comfort of the patient. Surgery is then completed.
Postoperatively, patients receive tobramycin and dexamethasone ophthalmic suspension 0.3%/0.1% (Tobradex, Novartis) and apraclonidine ophthalmic solution 0.5% (Iopidine, Novartis) 5 mg/5 mL immediately postoperatively. I prescribe topical nepafenac ophthalmic suspension 0.3 mg/mL (Nevanac, Alcon) once daily for 4 weeks postoperative.
CONCLUSION
After laser fragmentation, in most cases it is not necessary to divide nuclear pieces with great force, as the lenses are very often soft. My Femto Spoon is well adapted to this situation. Because it has no cutting edges or sides, there is no risk of harm to the lens capsule. When we do encounter very hard nuclei, the laser is not able to divide these lenses in the center. Current femtosecond laser technology cannot cut through opaque tissue. For these cases, the older Haefliger Phaco Cleaver can be used to crack nuclear pieces completely in the center of the capsule.
