




Descemet membrane endothelial keratoplasty (DMEK) is indicated for patients with disease affecting the corneal endothelium, such as Fuchs endothelial dystrophy and pseudophakic bullous keratopathy. Conventionally, these conditions were treated with penetrating keratoplasty, but the advent of endothelial keratoplasty over the past decade has led to improvements in both refractive outcomes and graft survival rates. Unlike Descemet-stripping automated endothelial keratoplasty (DSAEK)—in which the diseased layer of endothelium is replaced with a mechanically prepared endothelial graft containing a posterior stromal component—DMEK involves selectively replacing the Descemet membrane (DM) and the endothelium alone. The elimination of this posterior stromal component, which can be irregular in shape, reduces not only posterior astigmatism but also the incidence of graft rejection, and it results in faster visual recovery.1,2
Despite the potential for improved clinical and refractive outcomes with DMEK over DSAEK, the technical difficulties encountered with DMEK have led many surgeons to continue to choose DSAEK as their technique of choice in the treatment of posterior lamellar disease. In particular, intraoperative manipulation of the graft in the anterior chamber (AC) can be challenging, and excessive manipulation may lead to endothelial cell loss and cystoid macular edema. For this reason, there is a drive to standardize the surgery with a technique that minimizes intraoperative manipulation. Pull-through DMEK was developed as a result of this drive, and in this article we describe five fundamentals for its performance.
HOW PULL-THROUGH DMEK IS DIFFERENT
The preparation of DMEK tissue involves manually peeling the DM from the posterior stroma. Once the DM is free, it has a natural tendency to scroll into a configuration in which the endothelial layer is on the outer surface of the scroll. In pull-through DMEK, the graft is delivered into the AC in a controlled manner, whereby the graft naturally unfolds to match the posterior corneal contour. Rather than allowing the graft to scroll into its natural endothelium-out configuration, it is manually trifolded with the endothelium in. The graft is then inserted into the AC, and its natural tendency to open endothelium-out means it naturally apposes the posterior corneal surface readily, without manipulation (Figure).3
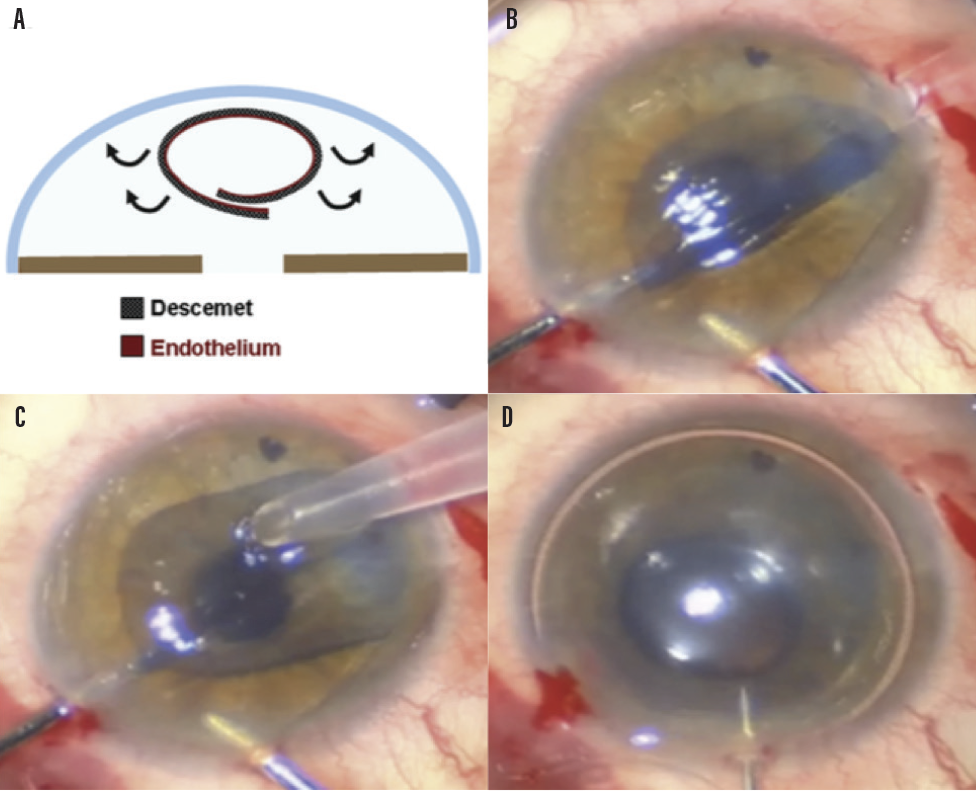
Figure. Schematic representation (A) and intraoperative photographs illustrating graft delivery and attachment (B–D). The natural tendency of the DMEK graft to roll with the endothelium outward (B, C) makes it unfold spontaneously under minimal irrigation from the anterior chamber maintainer. After unfolding is completed, air is injected under the DMEK graft until the anterior chamber is completely full (D).
Courtesy of James Myerscough, MD
1. RECIPIENT PREPARATION
Recipient preparation is, broadly speaking, the same process used in preparing a patient for conventional endothelial keratoplasty. There are four key steps to get right when preparing the recipient patient for the donor graft.
Step No. 1: Optimize visualization.Visualization is extremely important during the pull-through DMEK procedure. If the epithelium itself is edematous, it is imperative that the epithelium be removed to ensure a good view and to allow the cornea to quickly reepithelialize with new healthy cells.
Step No. 2: Stabilize the AC. The options for establishing AC stability while performing a descemetorhexis are to perform it under one of the following: air, aqueous with an AC maintainer, or an OVD. We strongly recommend performing descemetorhexis under air, and indeed that is the only way we perform it. Performing this maneuver under air provides far better visibility than the other media. Additionally, and specifically in the context of DMEK, having any viscoelastic material in the anterior chamber should be avoided because an OVD in the interface is likely to increase the risk of postoperative detachment of the graft and can cause haze that can persist for several months after surgery.
Step No. 3: Fully remove the peripheral endothelium. Any overlap of the donor graft over peripheral remnants of host DM is likely to increase the risk of detachment.
Step No. 4: Perform a PI.There are reports of successful endothelial keratoplasty without peripheral iridotomy (PI), but in our opinion, a PI is mandatory because it allows a full air fill to be performed. If a PI is performed, then the lower meniscus of the air bubble must be above the superior height of the PI rather than the pupillary margin postoperatively. The patient can, therefore, have a tighter air fill for a longer period of time than would be possible without a PI. The PI can be done either at the time of scheduling the patient for surgery, in clinic with an Nd:YAG laser, or manually at the time of surgery.
2. DONOR PREPARATION
We use prestripped corneas from an eye bank to perform this procedure. The techniques for stripping corneas and preparing the donor tissue have been described previously.4 In broad terms, to prepare a donor cornea, the tissue should be prestripped and punched to a diameter of 9.5 mm. The donor cornea is stripped, leaving an area of about 30°, or 1 clock hour in diameter, unstripped. This 30° unstripped area is marked with a pen at the limbus to keep the orientation obvious. Upon receipt of this corneal tissue from an eye bank, the endothelium has been repositioned back onto the posterior stroma. Before surgery, we punch it to a diameter between 8.25 and 8.75 mm, depending on the size of the recipient cornea and whether the patient has peripheral pathology. For patients with pseudophakic bullous keratopathy, we tend to slightly oversize the graft because the peripheral endothelium is likely to be pathologic, which is not necessarily the case in Fuchs endothelial dystrophy.
3. GRAFT INSERTION
We use forceps to manually trifold the edges of the donor graft inward. We then stain the graft again with trypan blue dye. We use endoforceps to pull the graft onto a soft therapeutic bandage contact lens, and then, using the same forceps, drag the graft (still in its trifolded configuration) into a commercially available IOL cartridge prefilled with balanced saline solution. Next, using the endoforceps that are already inserted through the opposite side of the cornea via a paracentesis, we insert the IOL cartridge into the eye, grasp the DM, and pull it into the center of the AC. Finally, we carefully remove the IOL cartridge to deliver the graft bimanually under low-flow infusion from an AC maintainer.
Once the graft is in the eye, the descemetic side of the unfolded DMEK graft, which was in contact with the IOL cartridge ceiling, should now be against the internal stromal surface of the recipient. We gently tap on the apex of the cornea to cause a natural unfolding of the donor tissue.
Graft failure, even in attached DMEK grafts, often occurs because the graft was inserted upside down. We strongly recommend that you mark the cornea before the procedure to ensure that you can tell whether the graft is upside down intraoperatively.
4. GRAFT TAMPONADE
We then perform a 100% full air fill. The air is inserted through the sideport incisions with a 27-gauge cannula. The cannula is advanced under the donor tissue to the center of the pupil, and the AC is filled with air. To ensure a tight air fill, air is injected under pressure using a 32-gauge needle inserted through the limbus. The needle is then retracted rapidly to prevent reflux.
In the recovery room, the patient is instructed to lie on his or her back for 2 hours, after which a slit-lamp examination is performed. By this point, the inferior meniscus edge of the air bubble is often already above the superior margin of the PI. If it is not, a small volume of air is gently burped from the AC at the slit lamp from one of the paracenteses using an AC cannula.
5. POSTOPERATIVE CARE
Patients should be admitted for 2 nights and prescribed dexamethasone and antibiotic drops to be administered four times a day. The patient is examined daily. If there is any graft detachment, it is best to have a very low threshold for immediate rebubbling with air or sulfur hexafluoride (SF6) gas. After the first two postoperative visits at days 1 and 2, the patient can be discharged and should be seen again after 1 week.
CONCLUSION
The technical difficulty in both graft preparation and surgical technique for pull-through DMEK has created a barrier that has prevented surgeons in both the United States and Europe from adopting and employing the technique. We hope that the five key points outlined here prove to be helpful to any surgeon looking to add pull-through DMEK to his or her armamentarium.
1. Gorovoy MS. Descemet membrane endothelial keratoplasty. Cataract & Refractive Surgery Today. https://crstoday.com/articles/2014-jul/descemet-membrane-endothelial-keratoplasty/. Accessed February 6, 2020.
2. Hindman HB, Huxlin KR, Pantanelli SM, et al. Post DSAEK optical changes: A comprehensive prospective analysis on the role of ocular wavefront aberrations, haze, and corneal thickness. Cornea. 2013;32(12):1567-1577.
3. Busin M, Leon P, Scorcia V, Ponzin D. Contact lens-assisted pull-through technique for delivery of tri-folded (endothelium in) DMEK grafts minimizes surgical time and cell loss. Ophthalmology. 2016;123(3):476-483.
4. Parekh M, Ruzza A, Ferrari S, Busin M, Ponzin D. Preloaded tissues for Descemet membrane endothelial keratoplasty. Am J Ophthalmol. 2016;166:120-125.



