

My routine cataract surgery technique includes the use of a femtosecond laser (LenSx, Alcon) in 99% of cases. As you can see in the Eyetube video that accompanies this article (bit.ly/carones0220), I first align the fragmentation and the capsulotomy and position the incision using the laser’s software and display. I prefer a 2.2-mm main incision in routine cases.
Once this is done, I check the anterior capsulotomy to make sure that it will be perfectly executed. I then determine the thinnest point of the crystalline lens in order to make sure that the fragmentation action of the laser within the nucleus will preserve the posterior capsule. Then I perform final checks of the anterior capsule and the placement of the main incision.
With the preliminary work complete, I start the action of the laser. Capsulotomy comes first, taking about 10 seconds. The laser then moves on to the nucleus fragmentation. In the video, you can see the pattern that I like being created, with concentric rings and four radial lines that will later facilitate quadrant division. The final action of the laser is the creation of the main incision.
The femtosecond laser is highly consistent and very accurate. Once this stage is complete, the patient is moved to the Lumera operating microscope (Carl Zeiss Meditec).
ENTRY AND NUCLEUS REMOVAL
I first create sideport incisions on either side of the main incision. I like to open my sideports using a 23-gauge blade because this allows me to place them accurately (Figure 1). I then inject an OVD, and the one that I prefer for all my routine cases is the viscous-dispersive DisCoVisc (Alcon).

Figure 1. A sideport incision is opened with a 23-gauge blade.
With the eye filled with OVD, I then use a blunt spatula (Janach) to check that the main incision is completely open and to verify that the anterior capsulotomy is free-floating. Once this is done, I lift the central part of the free anterior capsule with the spatula and then switch to forceps to remove the anterior capsule.
I perform hydrodissection and then I rotate the nucleus in the capsular bag to free it from adhesions.
The next step is nucleus and cortex emulsification and aspiration. As I mentioned earlier, the pattern delivered by the femtosecond laser allows me to create a very soft area in the center of the nucleus that I can remove quite easily with a very low amount of ultrasound. The separation of the four quadrants is also easily achieved. For these maneuvers, I use a femtosecond spatula (Janach) designed for this purpose. I hold the spatula with my right hand, and you can see in the video how easy it is to separate the four quadrants while I just carve the central portion of the nucleus with very low ultrasound.
Once the nucleus division is complete, I take advantage of the highly efficient fluidics of the Centurion Vision System (Alcon) to aspirate the nucleus quadrants as well as the epinucleus. Again, this maneuver is straightforward and easy in routine cases.
CORTEX REMOVAL
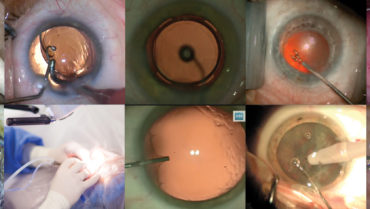
With quadrant removal complete, the next step is aspiration of cortical material that is stuck to the capsule (Figure 2). I have found that the cortex adheres much more adamantly to the capsule in eyes that have had femtosecond laser treatment, compared with eyes undergoing traditional cataract surgery. I like to use bimanual irrigation and aspiration because it allows me to reach every area around 360° of the capsule.
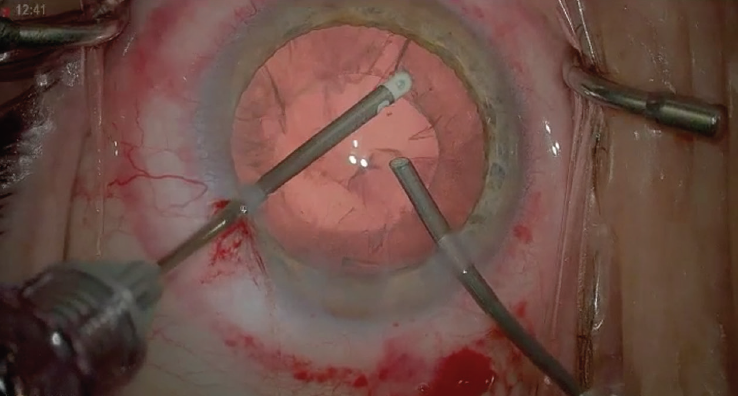
Figure 2. Cortical material that is stuck to the capsule is aspirated.
Once all the cortex is removed, I polish the posterior capsule using the soft and gentle tip of the aspiration cannula. I also polish the posterior surface of the anterior capsule to ensure that all the lens material is removed from the capsular bag.
IOL INSERTION AND CLOSING
Before IOL insertion, I again fill the capsular bag and anterior chamber with DisCoVisc, which, as I already mentioned, is my favorite OVD for all maneuvers. Once this is done, I am ready to implant the IOL. In the case shown in the video, the IOL is an AcrySof IQ Vivity (Alcon). I use a bimanual maneuver with a second instrument, in this case a Buratto nucleus manipulator, to stabilize the eye.
With the lens delivered into the capsular bag, I use the second instrument to help unfold the haptics faster in order to shorten the surgery time (Figure 3). Once the haptics are reasonably well unfolded, I begin to remove the OVD material, starting from the posterior capsular bag beneath the IOL. I try to be cautious to remove all the OVD from the posterior side of the IOL before I move to the anterior side of the IOL. I continue until all the OVD is removed.
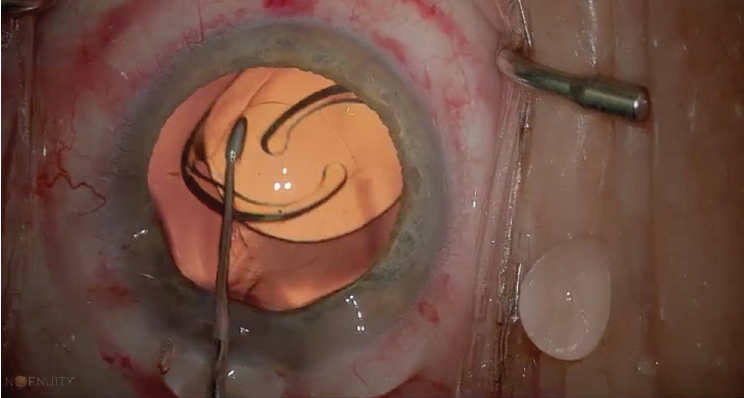
Figure 3. The second instrument is used to help unfold the haptics.
I don't use stitches for closure in 99% of cases. I just use wound hydration, or as I say, hydro-suturing, to close the wound. This is my standard surgery technique, which I do in all of my routine cases.
At the end of the surgery, I inject intracameral vancomycin, and I prescribe fluoroquinolone and dexamethasone eye drops for 1 week and diclofenac sodium eye drops for 1 month.
CONCLUSION
Some might not consider the use of the femtosecond laser for cataract surgery as routine, but in my case, I do. I use the laser in nearly every cataract surgery procedure, as I find that it is highly consistent and very accurate for the fragmentation, capsulotomy, and main incision portions of the procedure. The key to my routine cataract case is a quick, efficient, and, of course, safe surgical technique.
