
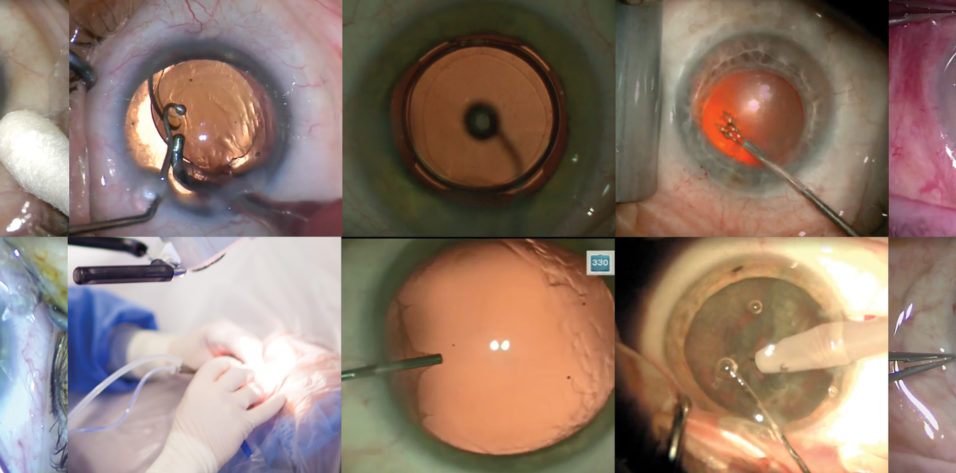

Cataract surgery has changed dramatically in the past few decades. And with each change, I have made certain tweaks to my routine procedure. Nowadays, I consider laser cataract surgery routine. A recent case, depicted in an accompanying Eyetube video (bit.ly/breyer0220), serves as an example of my standard surgical technique. The video also shows a routine manual phacoemulsification cataract surgery case.
MACHINES AND MATERIALS
The lens. One mainstay of my routine procedure is to ensure that patients experience gains in vision without disturbing photopic phenomena. In our practice, we mainly use extended depth of focus (EDOF) IOLs. When a patient presents with astigmatism, we always try to correct it during surgery, usually with the Lentis Comfort Toric (Oculentis) EDOF IOL, which can be custom ordered. One benefit we have found using this IOL is that, even when we do not meet the exact intended refraction, patients are still happy with their outcomes.
The laser. I perform laser cataract surgery in every case. I use the Lensar Laser System (Lensar) to perform the capsulotomy, to fragment the nucleus, and to finish with nonperforating astigmatism-correcting corneal incisions. The femtosecond laser is especially useful for performing astigmatic keratotomy (AK) in eyes with up to 1.00 D of astigmatism. In eyes with more than 1.00 D of astigmatism, I use the IntelliAxis-L marking system (Lensar) to help align the toric IOL.
The laser is located right outside the OR, so the patient undergoes the laser portion first and is then guided to the operating table to undergo the surgical portion of the procedure.
The phaco machine. I use the Centurion Vision System (Alcon), which I think right now is the best phaco machine on the market. Its anterior chamber stabilization system allows me to completely adapt the settings to my own needs. I use the OS 4 surgical platform (Oertli Instrumente) if I expect to perform a combined cataract–pars plana vitrectomy procedure in difficult cases.
The microscope. My favorite microscope is the Lumera 700 (Carl Zeiss Meditec). We attach a recording system to the microscope so that we can document every surgical case.
Other devices. We use the Cassini Videokeratographer (Cassini Technologies) to measure the anterior and posterior cornea and to perform iris registration. The data are transferred via WiFi or USB stick to the Lensar Laser System. While the patient is lying under the laser, the iris registration is checked and cyclotorsion is corrected so that either marks on the cornea or, even better, tabs on the laser capsulotomy can be used for orienting the toric IOL if one is used.
ROUTINE PROCEDURE, TWO WAYS
In most routine cases, patients receive peribulbar anesthesia. My surgical tool cart is pictured in Figure 1. It includes the sterile drape, blunt foil incision scissors, the eyelid speculum, a 2.4-mm double-blade bevel knife, a 1.1-mm paracentesis knife, cotton swabs and gauze, a methylcellulose OVD, a 3-mm syringe for hydrodissection and hydrodelineation, a needle holder, and my phaco tip, among other tools.
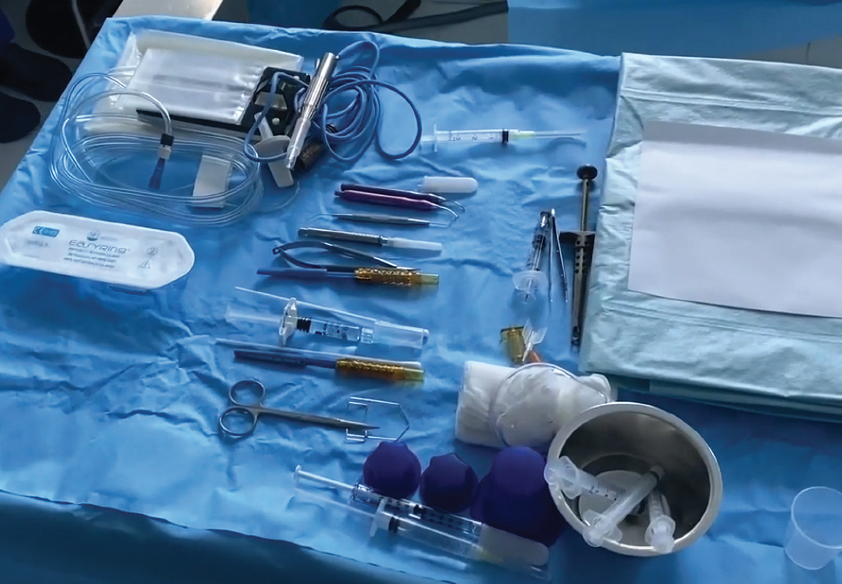
Figure 1. Dr. Breyer’s surgical tool cart.
Manual cataract surgery. First I instill the methylcellulose OVD into the anterior chamber and on top of the cornea, which keeps me from having to rinse the corneal surface throughout the procedure. I create the main incision on the steep meridian or, when the Lensar laser is used for AK, on the temporal line. I use a 2.4-mm double-blade bevel knife, but I push it only partway into the conjunctiva so that I end up with a 2-mm incision, which helps to reduce my surgically induced astigmatism to zero.
As I create the incision, I place a cotton swab on the other side of the eye to stabilize it during this step. I prefer the cotton swab to forceps because it helps me to avoid a subconjunctival hemorrhage.
Next I create 1.1-mm paracentesis incisions at the 11 and 1 clock hours, followed by a continuous curvilinear capsulorhexis created manually with a bent needle (Figure 2). In the manual cataract surgery case shown in the video, I implanted a plate-haptic IOL, and, therefore, my rhexis diameter was around 6 mm.
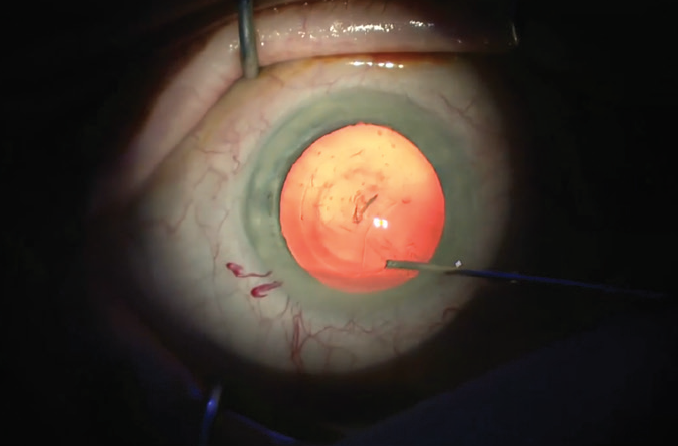
Figure 2. A bent needle is used to create the capsulorhexis.
For hydrodissection, I use a 3-mm syringe because I like its higher volume and greater diameter compared with typical hydrodissection and hydrodelineation cannulas. I like to ensure mobility of the nucleus by rotating it at least 180º to 190º.
Sitting at the 12 clock hour position, I perform phacoemulsification with my left hand in left eyes and with my right hand in right eyes. I usually use the continuous mode on the Centurion, with longitudinal phaco energy set to 0%. I prefer to use torsional energy, set to a maximum level of 70%. IOP is set at 46 mm Hg, vacuum rise up to 500 mm Hg, and aspiration to 40 mL/min. In a rock-hard nucleus, I still use continuous mode, but I add longitudinal ultrasound up to 60% phaco power, and torsional phaco power can go up to 100%.
As I begin the nucleus removal, I adjust the phaco tip, remove the anterior cortex, and perform a phaco stop-and-chop procedure. After the first nucleus division is made, I check that I have completely separated the two halves. Then I turn the nucleus 90º and create another division, and then emulsify and aspirate the four pieces of the nucleus in turn.
After nucleus removal, I perform bimanual irrigation and aspiration with the Centurion or the OS 4 using the following settings: IOP is set to 55 mm Hg, vacuum rise up to 500 mm Hg, and aspiration to 45 mL/min.
With all of the cortex removed, I inject a hyaluronic acid OVD (Carl Zeiss Meditec) into the capsular bag, followed by a capsular tension ring. I use this device in all premium lens surgeries to avoid the formation of striae in the posterior capsule, which can result in photopic phenomena for the patient. I remove the OVD, stabilize the eye with the irrigation infusion cannula in one hand and, with my contralateral hand, inject the IOL. Lastly, I hydrate the paracenteses and main incision.
Laser cataract surgery. Before I begin the phacoemulsification in a laser case, I perform thorough hydrodissection and hydrodelineation, just as I do in nonlaser cases. I then ensure that I can completely rotate the nucleus (Figure 3). When the nucleus can be rotated 360º after hydrodissection and hydrodelineation, the later process of cortex aspiration is usually made much easier.
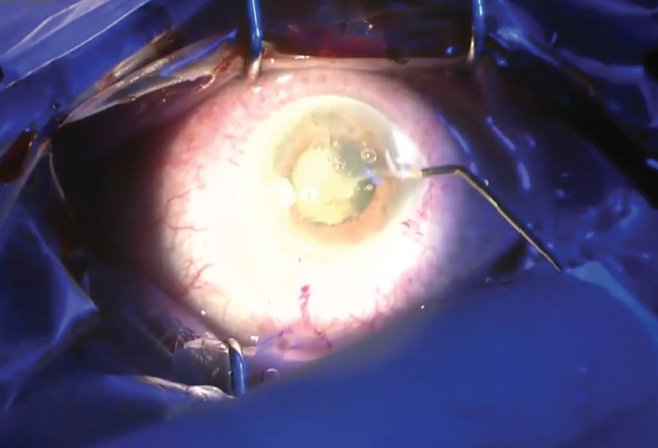
Figure 3. The nucleus is rotated after hydrodissection.
I love to use a stop-and-chop phaco technique with laser cataract surgery because it allows me to steer clear of the posterior capsule. It is easy to divide the nucleus in these cases because it was prechopped by the femtosecond laser.
After I remove the OVD, I inject the IOL under irrigation; this acts as counterpressure for the eye. Perhaps the best way to implant an IOL during laser cataract surgery is to anchor it to the capsulotomy. As you can see in my video, I implant the Femtis Comfort IOL (Oculentis), which is designed for rhexis fixation, into the capsular bag. I then pull all four special fixation haptics in front of the capsulotomy, so that it is anchored in the capsulotomy (Figure 4).
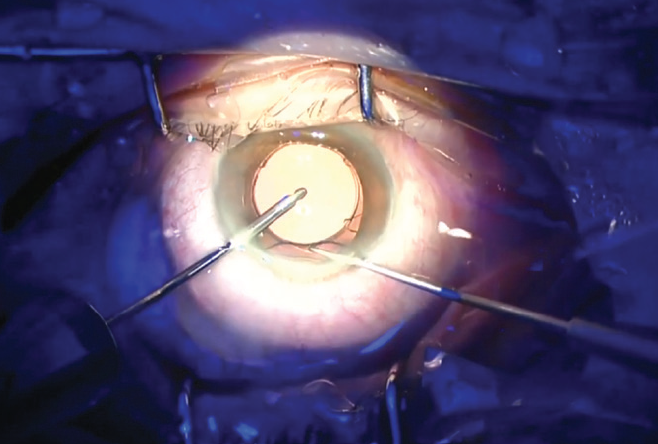
Figure 4. The Femtis IOL is enclaved in the capsulotomy.
At the close of surgery, I inject cefuroxime (Aprokam, Thea Pharmaceuticals), I hydrate the paracenteses and incision, and I inject dexamethasone and gentamicin under the conjunctiva.
CONCLUSION
My definition of routine cataract surgery has evolved over time. In the accompanying video, I share my routine manual cataract surgery technique, but nowadays what I really consider to be my routine procedure of choice is laser cataract surgery.
