


CASE PRESENTATION
A 91-year-old woman with hypertension experienced complications after cataract surgery. The patient’s medical history is significant for a cerebrovascular accident.
Preoperatively, BCVA was 20/40 OD and 20/50 OS with +3.25 D of spectacle correction. The patient had bilateral cortical cataracts and macular drusen. She underwent cataract surgery on the left eye 5 months ago. The surgeon implanted a preloaded hydrophilic acrylic Micro+ AY 123 with a yellow filter (PhysIOL, not available in the United States) through a 2.4-mm incision. The operation and postoperative period were uneventful. The manifest refraction after surgery was -0.5 -0.5 x 180º = 20/25.
Two months later, the patient underwent cataract surgery on the right eye using the same technique and lens implant. One day after surgery, the patient reported pain and impaired vision. An examination revealed a corneal erosion and diffuse, slight corneal edema. Cells were detected in the anterior chamber but no flare, fibrin, or hypopyon. The pupil was reactive but still partially dilated. The iris appeared to be normal, and there was no visible reaction in the vitreous. IOP measured 38 mm Hg, and BCVA was 20/63.
On postoperative day 2, the erosion had healed. Slight edema remained in the corneal stroma. Some cells were evident in the anterior chamber but no fibrin.
On postoperative day 3, the patient presented with visual acuity of 1m/25. IOP was 18 mm Hg. Although the corneal edema had decreased, fibrin was present in the anterior chamber, and seclusio pupillae with a fibrin membrane was observed in front of the IOL. The patient stated that the eye was no longer painful, and a B-scan showed no vitreous changes (Figure 1).
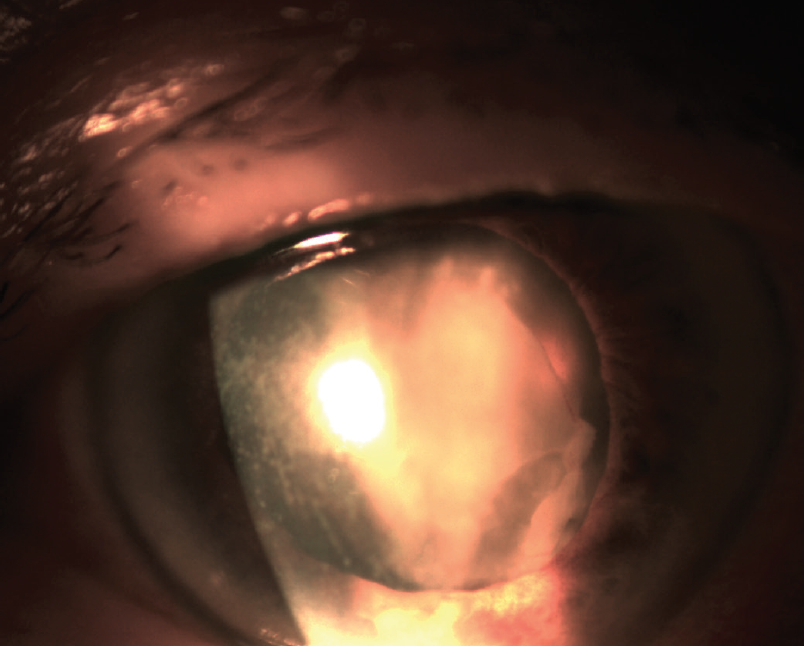
Figure 1. The eye’s appearance 3 days after cataract surgery.
How would you proceed?
—Case prepared by Magda Rau, MD

GERD U. AUFFARTH, MD, PHD, FEBO
My first thought is a diagnosis such as toxic anterior segment syndrome (TASS). Endophthalmitis, however, cannot be completely ruled out at this stage, so further evaluation is required. The appearance of fibrin on a hydrophilic IOL—especially after an IOP spike and the development of posterior synechiae—is not rare.
I would initiate treatment with topical and systemic steroids. Pupillary dilation and the administration of topical and systemic antibiotics may also be advisable because endophthalmitis cannot be excluded at this point. Recovery usually occurs in a few days, but the membrane sometimes remains for quite a while longer. Surgical intervention such as an injection of recombinant tissue plasminogen activator and/or simple irrigation and aspiration of the anterior chamber with an antibiotic included in the irrigating solution could be considered.
Another possibility is that residual cortex or nuclear fragments under the iris on the zonular plane caused the IOP spike and inflammatory reaction. If this is the situation, surgical aspiration with removal of the residual lens material is advisable. Treatment with topical and systemic steroids would help to stabilize the eye.


RAPHAEL PENATTI, MD; AND GEORGE O. WARING IV, MD, FACS
Although the reported incidence of endophthalmitis is as low as 0.03% to 0.2% worldwide,1 surgeons should maintain a high index of suspicion for this potentially devastating condition. Endophthalmitis typically manifests during the first 2 postoperative weeks, usually 3 to 5 days after cataract surgery.
The onset of TASS is typically 12 to 24 hours after cataract surgery, but this condition has been reported to develop as late as 160 days postoperatively.2
The anterior segment signs and symptoms of both conditions can include conjunctival hyperemia, corneal edema, hypopyon, pain, and impaired vision. Because vitreous changes are typical of endophthalmitis, their presence can facilitate the differential diagnosis, but it is important to note that such changes are also found in up to 23.8% of TASS cases.3
Given when this patient’s symptoms manifested, she most likely is experiencing TASS. We would therefore initiate treatment with a topical steroid such as 1% prednisolone acetate instilled four to eight times a day. For recalcitrant or more severe cases, a subconjunctival injection of dexamethasone or oral prednisolone is an option to control the inflammation, particularly if dense fibrin and hypopyon are present.
We would have a low threshold, however, for initiating empiric therapy of endophthalmitis with a vitreous tap and injection of broad-spectrum antibiotics.
Close observation of this patient is mandatory to ensure that the inflammation resolves. We would monitor her for improvement in visual acuity and pain relief. If the patient’s symptoms did not respond to treatment or worsened, we would consider surgical intervention such as chamber washout, vitrectomy, or IOL removal.

WHAT I DID: MAGDA RAU, MD
My initial diagnosis was TASS, but, because I could not rule out endophthalmitis, I initiated treatment for both conditions. Specifically, I prescribed topical therapy with diclofenac 0.1% administered four times a day, moxifloxacin 0.5% six times a day, dexamethasone every 2 hours, and a fixed combination of dorzolamide HCl and timolol maleate twice a day. The patient also began treatment with a systemic antibiotic and steroid. Additionally, I performed Nd:YAG laser therapy, which achieved only a round opening in the fibrin membrane because it was very dense. This opening facilitated later surgical intervention.
The next day, I opened the cataract incision, lifted the membrane slightly with forceps, and injected an OVD into the anterior chamber. To avoid damaging the zonular fibers and capsule, I performed gentle, mechanical removal of the membrane, followed by irrigation and aspiration.
I repositioned but did not rotate the IOL because it was already well centered. I then performed an intracameral injection of cefuroxime and subconjunctival injections of gentamicin and dexamethasone. The membrane was sent for bacterial examination.
One day after the membrane was removed, multiple additional fibrin fibers were visible in the anterior chamber (Figure 2, left). Treatment with an Nd:YAG laser was repeated, and visual acuity immediately improved to 20/50. The results of the culture were negative, so treatment with topical and systemic antibiotics was halted. Therapy with topical and systemic steroids was increased.
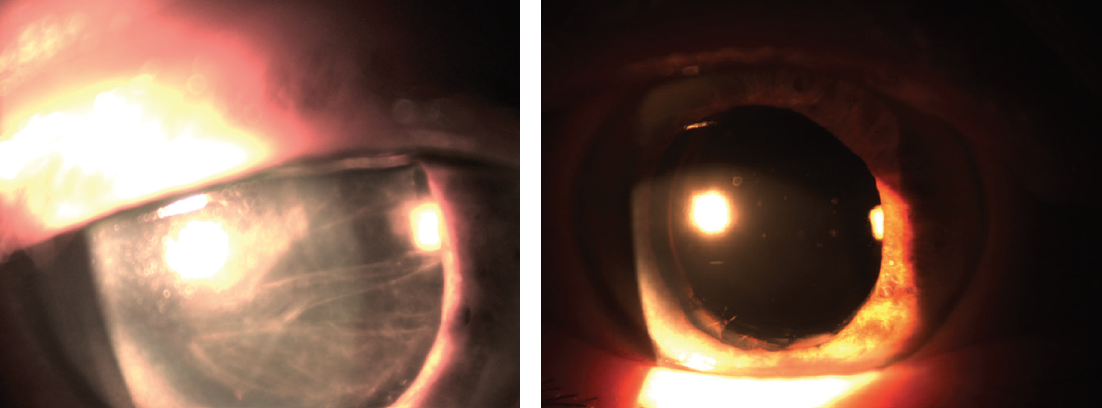
Figure 2. The appearance of the eye 1 day (left) and 3 weeks (right) after surgical removal of the membrane.
Two weeks after these interventions, UCVA was 20/40, and BCVA with a refraction of +0.50 -0.75 x 180º was 20/30. The cornea was clear, and no cells or flare was evident in the anterior chamber. The pupil remained dilated.
Three weeks after membrane removal, I treated the remaining synechiae between the iris and lens with an Nd:YAG laser, but the pupil remained dilated (Figure 2, right). Repeated applications of pilocarpine 1% had no effect; the iris was atrophic. The IOP on topical therapy was 17 mm Hg.
None of the other patients who underwent cataract surgery on the same day as this patient developed symptoms.
1. Garg P, Roy A, Sharma S. Endophthalmitis after cataract surgery: epidemiology, risk factors, and evidence on protection. Curr Opin Ophthalmol. 2017;28(1):67-72.
2. Miyake G, Ota I, Miyake K, Zako M, Iwaki M, Shibuya A. Late-onset toxic anterior segment syndrome. J Cataract Refract Surg. 2015;41(3):666-669.
3. Oshika T, Eguchi S, Goto H, Ohashi Y. Outbreak of subacute-onset toxic anterior segment syndrome associated with single-piece acrylic intraocular lenses. Ophthalmology. 2017;124(4):519-523.