


KEY TAKEAWAYS
- White cataracts with anterior capsular fibrosis can hide dangerous capsular tension despite a smooth preoperative appearance
- A mini-capsulorhexis, OVD support, blunt dissection, microscissors, and microforceps can release fibrotic adhesions while limiting radial tear risk
- Diffuse zonular weakness may require pressure equalization, low-energy phacoemulsification, fibrotic remnant removal, and sulcus placement of a three-piece IOL with optic capture

Often resembling a smooth summer moon, white cataracts can be deceptively beautiful under the microscope, but significant surgical challenges may lie beneath them. Sometimes, the anterior capsule is not only pressurized but also severely fibrotic, creating a complex situation in which performing the capsulorhexis becomes unpredictable and potentially dangerous. Successful surgery requires careful visualization, controlled decompression, and deliberate mechanical dissection of the fibrotic capsule.
This article uses a case example to highlight practical pearls for safely managing a white cataract with a fibrotic anterior capsule.
THE HIDDEN CHALLENGE
In the case example, the cataract initially had a smooth and uniform appearance at the surgical microscope, but the underlying pathology soon revealed itself.
The anterior capsule was stained with trypan blue dye under air to enhance visualization. Immediately afterward, severe corrugation of the capsule became evident, an early sign of significant underlying tension and fibrosis. The corrugation suggested that the anterior capsule was tethered by fibrotic adhesions to deeper structures of the lens (Figure 1).
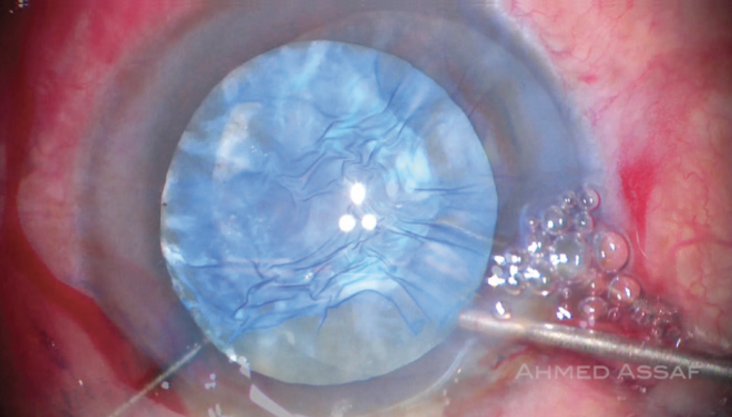
Figure 1. Trypan blue staining reveals corrugation of the anterior capsule in an eye with a white cataract and underlying fibrosis.
Such findings provide advanced warning that the capsulorhexis may not behave normally. Instead of tearing smoothly, the capsule may resist manipulation, or the tear may run unpredictably if the fibrous attachments are not addressed.
THE INITIAL MINI-CAPSULORHEXIS
After the excess dye was removed, a sequential injection of a dispersive OVD followed by a cohesive OVD was performed. This step served two purposes: it (1) maintained anterior chamber stability and (2) provided mechanical support to the fragile capsule.
The anterior capsule was then punctured to initiate the capsulorhexis. Instead of a full-sized tear, a small capsulorhexis was deliberately created initially. This allowed the surgeon to evaluate the pathology beneath the capsule while maintaining control over capsular tension.
Once the initial opening was created, a dense spider-like fibrous band was visible that was firmly adherent to the undersurface of the anterior capsule (Figure 2).
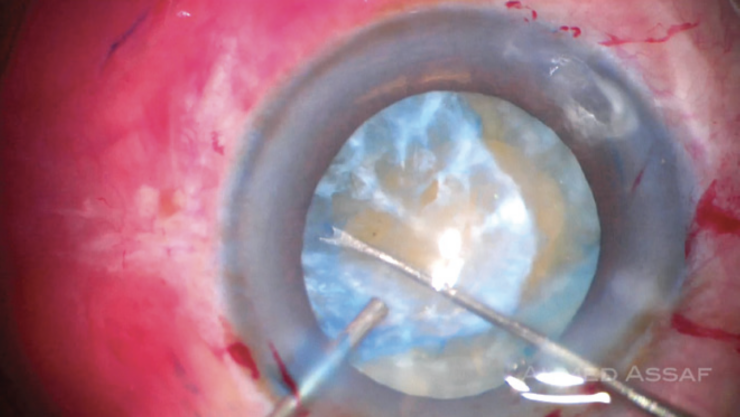
Figure 2. A dense spider-like fibrous band that has adhered to the undersurface of the anterior capsule is identified after the creation of a mini-capsulorhexis.
THE FIBROTIC NETWORK
Careful dissection was initiated with a blunt Y-shaped spatula and the continued support of a dispersive OVD. The goal was to separate the anterior capsule from the fibrous network beneath it.
Because the capsule was fragile, aggressive manipulation would have risked radial extension of the capsulorhexis. The dissection was therefore performed slowly and deliberately and extended as far peripherally as possible to release the fibrotic adhesions.
After most of the capsule had been freed from the fibrous band, the capsulorhexis was reinitiated. Microscissors were used to create a tangential cut, and microforceps were used to grasp the capsular flap and propagate the tear. The goal was to create a 5-mm capsulorhexis for better surgical access (Figure 3). In certain areas, however, the capsule could not be separated from the fibrotic adhesions. Microscissors were used to cut the anterior capsule and fibrotic complex circumferentially in these zones.
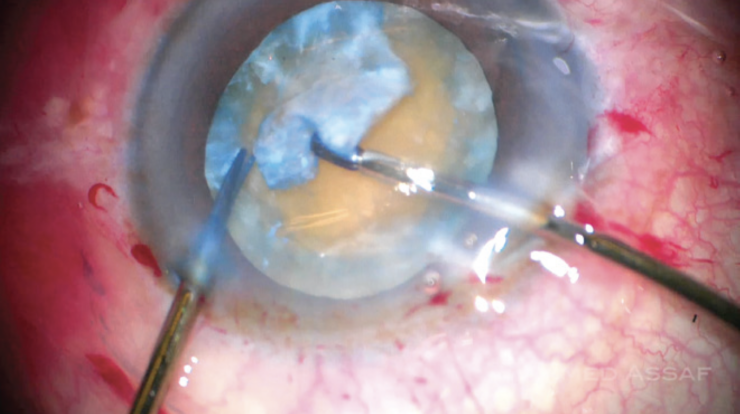
Figure 3. Dissection of the fibrotic complex beneath the anterior capsule.
THE FIBROUS BAND
Another injection of a dispersive OVD was performed to protect the capsule and maintain chamber stability. The fibrous band, once partially freed, was further dissected toward the periphery of the capsular bag. The thick, fibrotic tissue was then grasped with 23-gauge microforceps. Controlled traction and countertraction progressively separated this tissue from the anterior capsule, but the adhesions were too strong and the capsule too fragile to tolerate separation in some locations. In these areas, the fibrous band was carefully cut parallel to the edge of the capsulorhexis using microscissors. This allowed the central portion of the fibrotic complex to be removed from the anterior chamber (Figure 4).
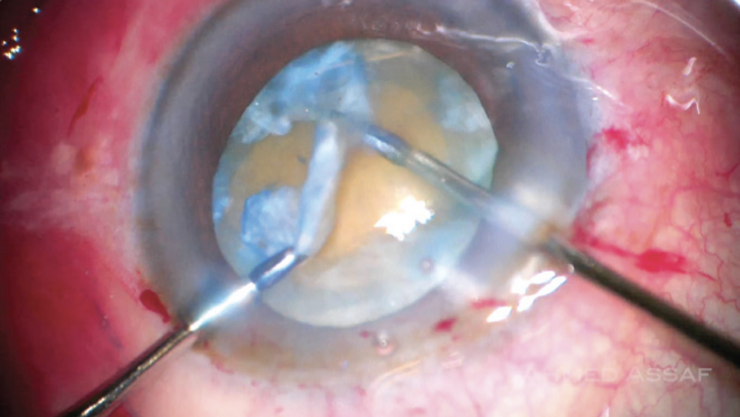
Figure 4. Controlled removal of the fibrotic band. Microforceps provide traction, while microscissors are used to cut the fibrous complex parallel to the edge of the capsulorhexis. The central fibrotic tissue is safely excised without extension of the capsular tear.
INTRAOPERATIVE INSTABILITY
Upon initiating irrigation with the phaco tip, lens–iris diaphragm retropulsion syndrome became evident, probably related to generalized zonular weakness (Figure 5). The iris was gently lifted away from the anterior capsule, which allowed the pressures between the anterior and posterior chambers to equalize. Once this balance was restored, surgery was able to proceed safely.
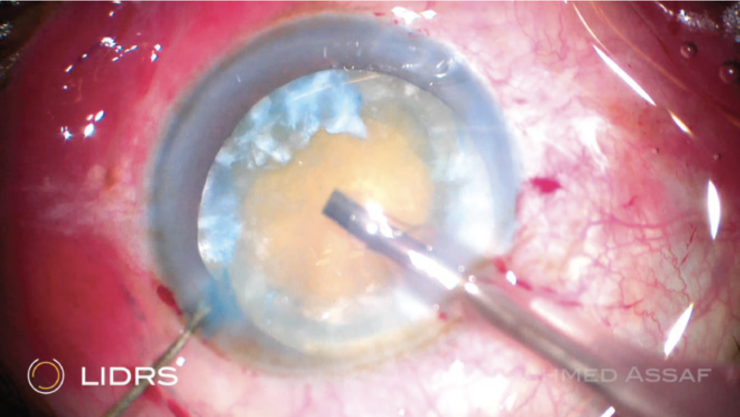
Figure 5. Lens–iris diaphragm retropulsion syndrome, likely secondary to generalized zonular weakness, is observed upon the initiation of irrigation with the phaco tip. The anterior chamber deepens, and the iris bows posteriorly, temporarily destabilizing the surgical environment.
This moment illustrates how complex cases like this one can be. Even routine surgical steps may provoke unexpected reactions when zonular integrity is compromised.
PHACOEMULSIFICATION
A quick-chop phaco technique was used to minimize ultrasound energy while emulsifying the dense nucleus. Following nuclear removal, residual cortex was aspirated from the capsular bag, which was then reinflated with a cohesive OVD. The remaining fragments of the fibrous band had become fully exposed. They were grasped with microforceps and excised with microscissors.
Removing these remnants is important for preventing future asymmetric capsular contraction that could distort the capsular bag or shift the IOL.
IOL STRATEGY
Given the diffuse zonular weakness and the fragile capsule, a three-piece IOL was selected for implantation. The IOL was placed in the sulcus with optic capture, providing additional stability and centration while protecting the compromised capsular bag. The main 2.8-mm incision was closed with a single 10-0 nylon suture (Figure 6).
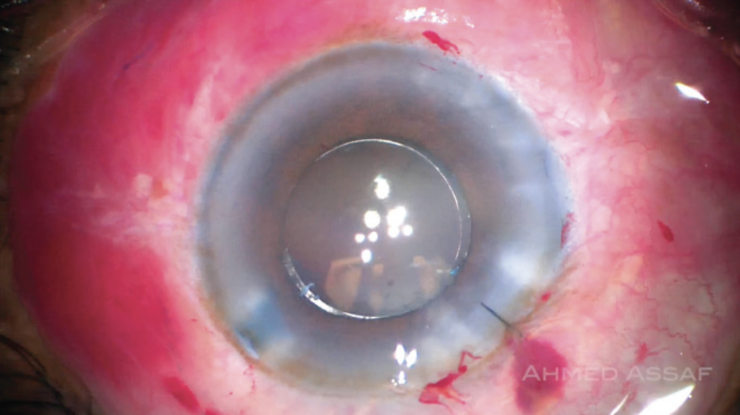
Figure 6. A three-piece IOL is placed in the sulcus with optic capture after removal of the fibrous complex.
POSTOPERATIVE OUTCOME
One week after surgery, the suture was removed. The eye had recovered well, and the visual axis was clear. What initially appeared to be a simple white cataract had concealed a complex fibrotic pathology beneath the surface.
With careful planning, controlled capsular management, and stepwise dissection, even challenging cases like this one can be managed successfully, creating a stable path toward visual rehabilitation.
An AI language model (ChatGPT, OpenAI) was used to assist with language editing. All content was reviewed, verified, and revised by the author, who assumes full responsibility for the accuracy and integrity of the manuscript. The AI tool was not used for data analysis, interpretation, or drawing scientific conclusions.
