


KEY TAKEAWAYS
- Secondary IOL fixation works best when astigmatism, white-to-white distance, conjunctival status, residual capsule, and corneal surgical plans drive technique selection
- With about 270º of capsular support, iris suture fixation can preserve existing anatomy and achieve stable optic capture
- Small-incision scleral suture fixation offers toric and centration control; Yamane or large-incision fixation can fit favorable anatomy or planned incisions


In our practice, small-incision scleral suture fixation (SSF) and flanged intrascleral haptic fixation (ISHF) with the Yamane technique1 are our primary posterior chamber IOL fixation strategies, but they are not our only options. Iris suture fixation (ISF) and large-incision scleral suture fixation of a CZ70BD IOL (Alcon) are valuable approaches and, in certain scenarios, may be preferable.
We do not view these techniques as competitors. The art lies not in mastering a single technique but in recognizing when to pivot from one to another.
WE START WITH ASTIGMATISM
The first question we ask is whether the patient is a candidate for a toric lens.
If the patient has reproducible corneal astigmatism of greater than 2.00 D and good visual potential, we favor small-incision SSF, which permits the off-label implantation of toric platforms such as the enVista (Bausch + Lomb). The strategy allows precise IOL centration when performed methodically; we can titrate suture tension intraoperatively and fine-tune rotational alignment in a way that is not currently possible with ISHF of a nonadjustable three-piece IOL using the Yamane technique.
Recently published case series have also described the ISHF of a Light Adjustable Lens (RxSight).2 This lens offers astigmatic correction, but in our experience, it also presents unique challenges with ISHF. The haptic-optic junction is fragile, residual tilt can occur, and, most importantly, a pupil size of less than 6 mm can affect postoperative light treatments.
Whenever astigmatic correction is a priority, we choose the fixation technique with astigmatism management in mind.
ANATOMY GUIDES THE PIVOT
Next, we evaluate white-to-white distance, residual capsular support, and overall ocular anatomy.
Three-piece IOLs fixated using the Yamane technique have haptic spans of approximately 13 mm. In larger eyes, that span may be insufficient for optimal long-term centration. If the white-to-white distance is large or scleral integrity is questionable, SSF offers greater flexibility than ISHF. Because lens position is determined by suture placement rather than haptic compression, centration can be customized regardless of globe diameter. Conversely, if there is significant conjunctival scarring from prior surgery, we tend to favor ISHF to avoid large conjunctival peritomies.
WHEN ISF IS ENOUGH
Before committing to secondary scleral fixation, we evaluate the capsule. If approximately 270º of capsular support remains, we strongly consider ISF. In these eyes, the remaining capsule can function as a structural scaffold. Rather than abandon that support entirely, we can leverage it.
ISF allows us to use the residual capsular architecture without placing the IOL fully in the bag. A three-piece IOL is placed in the sulcus, and the optic is prolapsed anterior to the pupillary margin via reverse pupillary capture. From there, a 10-0 polypropylene suture on a CTC-6 needle is passed through the midperipheral iris proximal to the haptic and then again distal to the haptic. The suture end is externalized and secured with the surgeon’s intraocular knot of choice (McCannel, Siepser sliding, or McAhmed).
The key is appropriate candidate selection. Without sufficient capsular support, sulcus placement with ISF risks progressive IOL subluxation and late dislocation. In a properly selected eye, however, ISF can be elegant, efficient, and remarkably stable. Whenever possible, we aim for optic capture through an intact capsulotomy for greater stability and centration. In our experience, when the anterior and equatorial zonules are intact, optic capture of an IOL is one of the most stable configurations short of placement in the bag.
WHEN SSF OFFERS THE MOST CONTROL
SSF requires meticulous suture handling and symmetric tensioning. We pass nonabsorbable PTFE sutures through the eyelets of an enVista IOL (model MX60E or MX60ET). We place the sutures at least 3 mm posterior to the limbus to avoid anterior positioning and lessen the risk of iris chafe and uveitis-glaucoma-hyphema syndrome (Figure 1).
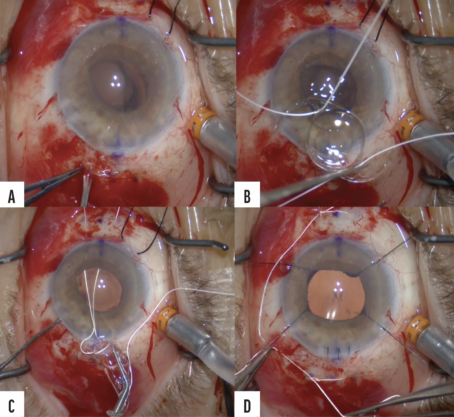
Figure 1. SSF of a foldable enVista MX60 IOL (off-label use). Scleral marks are placed 3 mm posterior to the limbus, and paired sclerotomies are created (A). PTFE sutures are passed through the eyelets and haptics (B). Sutures are externalized before lens insertion (C). The IOL is inserted and centered in a 2-1-1 knot configuration. The knots are buried to prevent erosion (D). Note: SSF and the use of PTFE suture are off-label in the United States.
SSF offers several advantages, including excellent IOL centration control. The strategy may be used with a toric IOL, and durability data beyond a decade are available for SSF.
The trade-offs are important to recognize. SSF requires symmetric tensioning and meticulous knot burial. Transient early hypotony is more common with SSF than with ISHF because suture fixation requires sclerotomies. There is also a rare risk of eyelet fracture or late suture erosion.
For surgeons who value predictable precision and long-term familiarity, SSF remains a highly reliable option.
WHEN A LARGE-INCISION OR SUTURELESS APPROACH IS PREFERRED
Although modern fixation techniques emphasize small incisions, the CZ70BD IOL is a time-tested option for secondary fixation.3-5 The 7-mm optic requires an equally large incision for implantation, but it also reduces the visual consequences of mild IOL decentration. For this reason, we typically reserve this IOL for patients in whom a large incision is already planned, such as when surgery is combined with penetrating keratoplasty, in eyes with midperipheral iris defects, or when a PMMA IOL is being removed.6 In these situations, the requirement for a large incision becomes irrelevant, and the stability advantage becomes compelling.
The Yamane and glued IOL techniques are sutureless and typically faster once proficiency is achieved. Avoiding scleral suture passes may lessen early wound-related hypotony and eliminate the risk of suture erosion. The learning curve is steep, however, and even highly experienced surgeons can encounter intraoperative challenges with IOL centration and tilt. In our practice, these are the most meaningful intra- and postoperative risks associated with these techniques. Recently, we developed the Crimper (Epsilon) to make tunnel length more consistent (Figures 2 and 3).
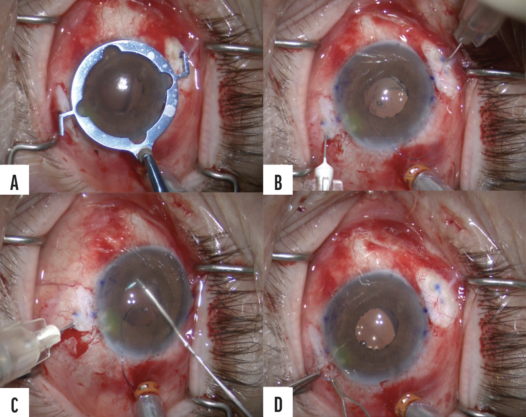
Figure 2. Double-needle flanged ISHF (Yamane technique) of a three-piece IOL. Scleral marks are placed 2 to 2.5 mm posterior to the limbus (A). Paired 30-gauge needles are used to create scleral tunnels (B). Haptics are docked and externalized (C). Low-temperature cautery is performed to create flanges, which are tucked into the tunnels (D). Note: Flanged ISHF and posterior fixation of three-piece IOLs without capsular support are off-label in the United States.
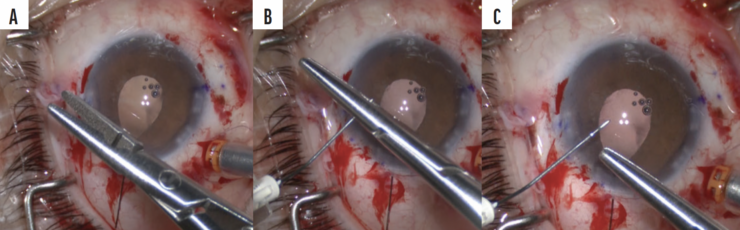
Figure 3. The Crimper allows a surgeon to insert the needle to mark or crimp exactly 2 mm of tissue to standardize tunnel length and the entry point into the eye.
The rotisserie tilt phenomenon7 at the haptic-optic junction of the CT Lucia 602 (Carl Zeiss Meditec) has influenced our lens selection during the past few years. Although the CT Lucia 602 has PVDF haptics that dock easily, we have transitioned to alternative platforms, such as the Sensar (model AR40e, Johnson & Johnson Vision) and SofPort (model LI61AO, Bausch + Lomb). Their PMMA haptics require more delicate handling to avoid kinking. When implanting an AR40e, we dock it in a maximum-diameter 30-gauge TSK needle. When placing an LI61AO, we use a regular thin-walled 30-gauge TSK needle.
Successful Yamane ISHF depends on precise needle entry 2 to 2.5 mm posterior to the limbus, symmetric scleral tunnel length, careful flange creation, and a peripheral iridotomy to reduce optic capture. IOL tilt typically results from asymmetric tunnel length or stress near the haptic-optic junction.
HOW WE MATCH THE TECHNIQUE TO THE EYE
In our practice, the overall complication rates for SSF and ISHF are comparably low. Our rate of cystoid macular edema with either secondary IOL fixation method is approximately 9%. Our patients are therefore evaluated by a retina specialist during the postoperative period. Interestingly, when ISF is performed in the presence of 270º of anterior capsular support, the cystoid macular edema rate is 3.8%.8 One difference we have observed is that our patients undergoing SSF tend to experience slightly earlier hypotony but require fewer reoperations than our patients undergoing ISHF. Lastly, ISHF, although promising, lacks the long-term durability data of SSF to establish noninferiority.9
We favor ISF when the following are true:
- At least 270º of capsular support is available;
- Optic capture is feasible; and
- There is a desire to preserve existing anatomy.
We favor small-incision SSF when the following are true:
- Significant corneal astigmatism warrants toric correction;
- The white-to-white distance is either very large or very small; and
- Maximal IOL centration control is required.
We favor large-incision SSF when the following are true:
- A large incision is already planned;
- Surgery is being combined with a corneal procedure; and
- Maximum long-term mechanical stability is desired.
We favor ISHF when the following are true:
- Ocular anatomy is favorable;
- Surgical efficiency is a priority;
- A toric IOL is not indicated; and
- Suture-related complications are a major concern.
CONCLUSION
Ultimately, secondary IOL fixation is not about choosing a single superior technique but about matching the method to the eye. In our experience, the most important determinant of success is not the method itself but the surgeon’s familiarity with its nuances. Even when capsular support is compromised, thoughtful decision-making can restore control and yield excellent outcomes.
1. Yamane S, Sato S, Maruyama-Inoue M, Kadonosono K. Flanged intrascleral intraocular lens fixation with double-needle technique. Ophthalmology. 2017;124(8):1136-1142.
2. Chen AJ, Rodgers EG, Wang L, et al. Visual and refractive outcomes with intrascleral haptic fixation of the Light Adjustable Lens. J Cataract Refract Surg. Published online March 10, 2026. doi:10.1097/j.jcrs.0000000000001936
3. Bonnell AC, Mantopoulos D, Fine HF, Shah SP, Wheatley HM, Prenner JL. One-year outcomes of a novel surgical approach for fixation of a posterior chamber intraocular lens using Gore-Tex suture. Retina. 2020;40(5):833-837.
4. Khan MA, Gupta OP, Smith RG, et al. Scleral fixation of intraocular lenses using Gore-Tex suture: clinical outcomes and safety profile. Br J Ophthalmol. 2016;100(5):638-643.
5. Pollmann AS, Lewis DR, Gupta RR. Structural integrity of intraocular lenses with eyelets in a model of transscleral fixation with the Gore-Tex suture. J Cataract Refract Surg. 2020;46(4):617-621.
6. Gouvea L, Din N, AlShaker S, et al. Clinical outcomes of transscleral-sutured intraocular lens combined with Descemet membrane endothelial keratoplasty. Cornea. 2023;42(12):1497-1502.
7. Enright JM, Purt B, Bruck B, et al. Severe spontaneous tilt of scleral-fixated intraocular lenses. Am J Ophthalmol. 2024;262:206-212.
8. Alsetri H, Masket S, Fram N, et al. Surgical outcomes of intraocular lens iris suture fixation in eyes with residual capsule support. J Cataract Refract Surg. 2024;50(4):407-412.
9. Chang CH, Hung JH, Chang YS, Lee YK. Comparison of flanged intrascleral haptic fixation and 2-point transscleral Gore-Tex sutured IOL fixation: a 12-month cohort study. J Cataract Refract Surg. 2026;52(3):383-391.
