


KEY TAKEAWAYS
- Dislocated IOL–capsular bag complexes should be preserved only when the IOL power, optic clarity, haptics, and capsular fibrosis are favorable
- A Goldilocks complex has enough fibrosis to hold lasso sutures but not enough contraction, Soemmering ring material, or lens damage to cause problems
- Dead bag syndrome, hydrophilic acrylic IOLs, damaged optics, or large Soemmering rings generally favor complete complex removal and Yamane intrascleral haptic fixation

With more patients undergoing cataract surgery at a younger age and living longer, we ophthalmologists are seeing an increasing number of dislocated IOL–capsular bag complexes, and that number is likely to continue to grow. In my referral practice, I see a few of these cases every week. I have had to learn how to manage them not only effectively but also efficiently and to develop surgical plans that will hopefully fix the patient in one surgery without a need for additional procedures down the road.
One of the key decisions in managing a patient with a dislocated IOL–capsular bag complex is whether to preserve the complex or replace it. In my practice, the trend has shifted toward removing and replacing the entire IOL–capsular bag complex with Yamane intrascleral haptic fixation (ISHF),1 but there are certain circumstances in which I will retain the existing IOL and either reposition it with optic capture or lasso the IOL–capsular bag complex to the sclera with CV-8 PTFE sutures (Gore-Tex, W.L. Gore & Associates).
WHEN I CONSIDER PRESERVING THE COMPLEX
The IOL–capsular bag complex I want to preserve is what I call the Goldilocks complex, in which there is just enough fibrosis of the capsular bag to hold the sutures on the haptics, not too much Soemmering ring material, and an IOL of the correct power with a clear, undamaged optic that is likely to remain clear over time.
When a patient presents to me with a dislocated IOL–capsular bag complex, one of the first questions I ask is, “Were you happy with your vision in that eye before the lens dislocated?” If the answer is yes, I am more likely to consider preserving that lens through repositioning.
It is also extremely helpful to know the lens model and IOL power. If old records or a lens card is available, that information is important to review. I then measure the patient with my biometer and compare the needed lens power with the power of the dislocated lens already in the eye to determine whether the IOL is the correct power and worth saving. In many cases, the dislocated lens can be seen at the slit lamp or on indirect ophthalmoscopy, and, to the extent possible, I try to determine whether the haptics are intact rather than kinked or contracted by capsular bag fibrosis and whether the optic is clear (Figure 1).
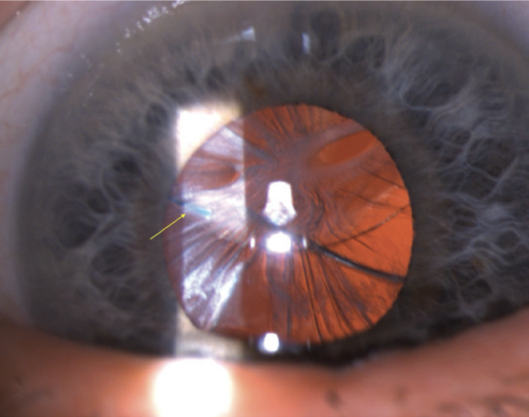
Figure 1. The yellow arrow indicates a haptic compressed by capsular bag contraction onto the optic surface. This haptic is likely damaged, and the bag is too contracted and phimotic for repositioning to be considered. The entire IOL–capsular bag complex was therefore removed and replaced with Yamane ISHF.
Many older hydrophobic acrylic lenses have significant glistenings or subsurface nanoglistenings, and if that is the case, I am inclined to remove the lens and replace it with a clear one. If I see that the lens is significantly pitted or damaged from a previous Nd:YAG laser capsulotomy, I remove it as well. If the dislocated lens is made of hydrophilic acrylic, I always exchange it because of the risk of future calcification after secondary surgery.
WHEN I PREFER AN EXCHANGE
Often, the IOL–capsular bag complex has dislocated onto the retina by the time the patient is ready for surgery. In that situation, I would rather hedge my bets and remove the entire IOL–capsular bag complex and replace it with Yamane ISHF. In my hands, an IOL exchange under these circumstances is actually easier and faster. Typically, the eyes are quieter as well because all potentially inflammatory Soemmering ring material is removed at the time of surgery.
The exception would be a toric lens of the correct power in a patient with significant astigmatism. If it is possible to fixate that complex to the sclera and preserve the benefit of the toric correction, I will try to do that if the IOL–capsular bag complex is amenable to lasso fixation (click here for a demonstration).
DEAD BAG SYNDROME
An increasingly common cause of IOL–capsular bag complex dislocation that I am seeing in my referral practice years after cataract surgery is dead bag syndrome.2 These are IOL–capsular bag complexes that, many years after the original surgery, show no capsular contraction or fibrosis. Instead, the capsular bag is thin, diaphanous, and devoid of lens epithelial cells. The bag dislocates because there is nothing of substance for the zonules to hold onto (Figure 2).
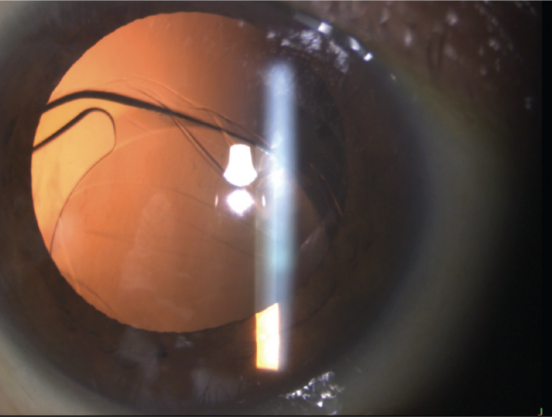
Figure 2. A dead bag dislocation that occurred a few years after cataract surgery. The capsular bag has no fibrosis or structural integrity, and because the zonules therefore have nothing to anchor onto, the IOL–capsular bag complex dislocates. In these cases, Dr. Safran prefers to remove and replace the complex with Yamane ISHF.
In dead bag syndrome cases, I always remove and replace the complex because, if I try to lasso it, the bag shreds and falls apart when sutures are passed through it, and the sutures do not hold. To securely lasso an IOL–capsular bag complex to the sclera by wrapping a PTFE or polypropylene suture around the haptics and fixating it through sclerotomies, there must be enough fibrosis of the bag to hold the suture on the haptic so that it does not slide off.
In dead bag syndrome, there is no structural integrity to the capsular bag, so the sutures tend to slide off the end of the haptic unless the haptic has an eyelet that can be used to hold the suture, in which case capsular bag integrity becomes somewhat irrelevant (click here for a demonstration).
THE PROBLEM OF SOEMMERING RING MATERIAL
Another indication to remove and replace the IOL–capsular bag complex is the presence of a large amount of Soemmering ring material within the bag. If the capsular bag is pierced to suture the complex and there is a great deal of this material present, it can leach into the eye and cause significant problems, including inflammation, secondary glaucoma, cystoid macular edema, and even corneal decompensation.
If I see a large Soemmering ring in the bag, I tend to remove and replace the entire complex, while taking care to remove all of the material. Often, the Soemmering ring comes out with the IOL–capsular bag complex under infusion pressure through the main incision. In other cases, some material falls back and must be retrieved and removed with the vitrector. In still other cases, the Soemmering ring is calcified or extremely large and dense and requires the fragmatome for complete removal (click here for a demonstration). It is imperative to remove all of this material from the eye, and when that goal is achieved, I find that the eyes are quiet in the postoperative period.
IN SUMMARY
The Goldilocks complex is an IOL–capsular bag complex that has dislocated but contains an IOL worth preserving and a capsular bag with just the right amount of fibrosis to hold lasso sutures on the haptics without too much fibrotic contraction or lens material that could create problems. In such a case, I lasso the complex to the sclera with a CV-8 PTFE suture, and I combine that with pars plana infusion and vitrectomy to avoid vitreous traction, maintain control, and manage bleeding and debris. (Click here for a demonstration.)
1. Yamane S, Sato S, Maruyama-Inoue M, Kadonosono K. Flanged intrascleral intraocular lens fixation with double-needle technique. Ophthalmology. 2017;124(8):1136-1142.
2. Culp C, Qu P, Jones J, et al. Clinical and histopathological findings in the dead bag syndrome. J Cataract Refract Surg. 2022;48(2):177-184.
