


KEY TAKEAWAYS
- Soemmering rings can cause IOL tilt, visual symptoms, glaucoma, endothelial decompensation, and vitreous opacities, making complete removal clinically important
- With an intact posterior capsule and in-the-bag IOL, OVD-assisted capsular separation allows ring dislodgement, anterior chamber delivery, and phacoemulsification
- With posterior capsule rupture, iris hooks, vitrector-assisted release, glued intrascleral haptic fixation, and iris barrier restoration help prevent vitreous cavity loss


After cataract surgery, a Soemmering ring can form when proliferating residual lens epithelial cells or residual cortex becomes trapped between the anterior and the posterior capsular flaps. Younger patients are at increased risk of developing a Soemmering ring due to fusion of the anterior and posterior capsules (Figure 1).
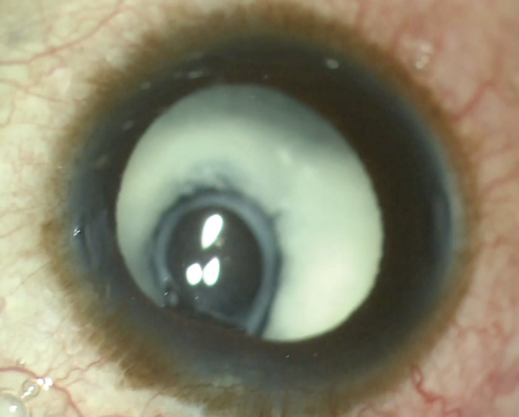
Figure 1. Microcornea with associated aphakia and a massive 360º Soemmering ring.
Removal of a Soemmering ring is essential because the material can cause significant IOL tilt, visual disturbances, and secondary complications such as secondary glaucoma, corneal endothelial decompensation, and vitreous opacities. Unfortunately, extraction can be tricky, and the strategy depends on the clinical scenario.
SCENARIO NO. 1
If the posterior capsule is intact and the IOL is in the bag, an OVD is injected in between the anterior and posterior capsules to create space. Next, a Sinskey hook is carefully used to dislodge the Soemmering ring and nudge it out of the capsular bag. The ring is then brought into the anterior chamber and emulsified with the phaco probe (Figure 2). Alternatively, lightly tapping the posterior lip of the corneal incision can cause spontaneous extrusion of the ring.
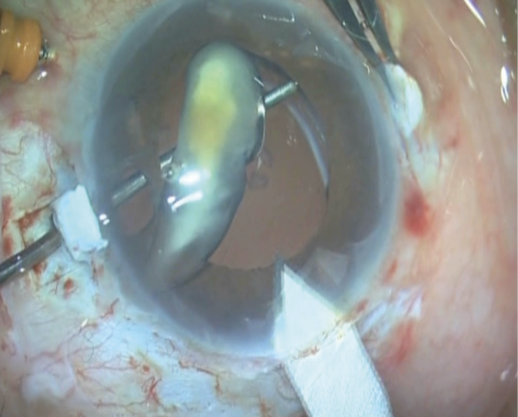
Figure 2. A Soemmering ring is elevated into the anterior chamber while supported by the passage of a rod to prevent the material from falling into the vitreous cavity. The limbal section is enlarged to facilitate the ring’s extrusion from the eye.
SCENARIO NO. 2
Management is more challenging if the posterior capsule has ruptured and the anterior and posterior capsules have fused together (Figure 3). In this situation, the Soemmering ring is typically located peripherally in the equatorial region of the capsular bag and is often hidden behind the iris. The placement of iris hooks can facilitate visualization.

Figure 3. A decentered three-piece IOL in the presence of a ruptured posterior capsule, optic capture, and Soemmering ring (A). The IOL is carefully disengaged from the iris. Two partial-thickness scleral flaps are made 180º apart, as would be done in a glued intrascleral haptic fixation procedure (B). Both haptics are externalized and tucked into the scleral pockets. The Soemmering ring is dislodged from the periphery and manipulated into the center of the capsular bag (C). The Soemmering ring is emulsified with the phaco probe (D).
Glued intrascleral haptic fixation of a secondary IOL is performed. Next, the Soemmering ring is carefully dislodged from the surrounding vitreous with the help of a vitrectomy probe. The vitrector cuts the adhesions surrounding the ring, eventually releasing it. The ring is then brought into the center of the capsular bag and emulsified with the phaco probe in a manner similar to an IOL scaffold procedure.
Throughout the procedure, there is a risk that the Soemmering ring could slip around the edge of the IOL optic and fall into the vitreous cavity. If this occurs, a complete posterior vitrectomy is warranted, followed by manipulation of the ring into the anterior chamber and the material’s removal from the eye.
A trick we use is to release the iris hooks after dislodging Soemmering ring and manipulating it into the center of the pupil. This can help the iris tissue resume its original state and form a physical barrier around the IOL, preventing the Soemmering ring from slipping into the vitreous.
CONCLUSION
The management of a Soemmering ring is challenging. Careful surgical planning and technique can achieve good visual outcomes in these eyes.
