


KEY TAKEAWAYS
- Secondary IOL fixation now spans sutured, flanged, glued, and purpose-designed platforms, making technique selection dependent on ocular anatomy and available capsular support.
- The Carlevale IOL shows how purpose-built scleral fixation can improve predictability, but it still requires IOL exchange and remains unavailable in some markets.
- Emerging devices such as the prosthetic capsular bag and Oseguera Ring aim to stabilize aphakic or dislocated IOL scenarios without relying on traditional sutures.

Aphakia and IOL instability in eyes without capsular support are among the most demanding scenarios for anterior and posterior segment surgeons. As the global volume of cataract surgery approaches 28 million procedures per year, late IOL dislocation, zonular failure related to pseudoexfoliation (PXF), posttraumatic aphakia, and intraoperative capsular rupture account for a growing number of complex cases. An estimated 1% to 2% of pseudophakic patients ultimately require secondary IOL fixation, translating to hundreds of thousands of cases worldwide each year.1
Managing these eyes requires technical versatility and a clear understanding of the advantages and limitations of each approach. During my training, including a year dedicated to retina and vitreous surgery alongside surgeons who had experience with the full range of secondary fixation techniques, I gained firsthand exposure to the field’s evolution. Suture-based methods provided effective fixation but carried the risks of late suture erosion and endophthalmitis, and sutureless flanged techniques reduced reliance on sutures. Purposefully designed platforms are being developed to improve long-term stability. This article reviews the major secondary IOL fixation techniques, places each in clinical context, and discusses two devices that could expand the options for this challenging patient population.
WHEN THE LENS WILL NOT STAY
Secondary IOL fixation is indicated whenever implantation in the bag or sulcus is not feasible and the eye cannot be left aphakic. The clinical presentations vary: late in-the-bag dislocation from progressive zonular weakness in PXF syndrome; posttraumatic subluxation or total aphakia; crystalline lens dislocation in patients with connective tissue disorders such as Marfan syndrome; pediatric aphakia after lensectomy; uveitis-glaucoma-hyphema syndrome from a malpositioned or unstable anterior segment lens; and intraoperative rupture of the posterior capsule with inadequate sulcus support.
Scleral-fixated IOLs can provide a physiologic posterior chamber alternative to anterior chamber IOLs and iris-fixated lenses in many of the aforementioned scenarios,2 particularly when endothelial reserve is limited, the anterior chamber is shallow, or the iris architecture is compromised. The challenge is selecting the best approach to each eye because no single technique answers every situation.
Sutured Scleral Fixation
Sutured scleral fixation using 9-0 or 10-0 polypropylene or PTFE sutures (off-label use) has the longest track record and the most longitudinal outcomes data of any secondary fixation method. IOLs with haptic eyelets, such as the Akreos (model AO60, Bausch + Lomb) for four-point fixation and the enVista (model MX60, Bausch + Lomb), allow stable anchoring at the ciliary sulcus level and work with a wide variety of eyes. PTFE sutures have increasingly replaced polypropylene sutures in some centers because the greater tensile strength of the former may lessen the risk of breakage; 10-0 polypropylene suture erosion or rupture has been reported in up to 27.9% of cases at long-term follow-up.3
Despite its limitations, sutured scleral fixation remains an important option in anatomically constrained eyes, such as those with scarred conjunctival tissue from glaucoma surgery, a fibrotic Tenon capsule, or a need for concomitant penetrating keratoplasty, where sutureless techniques are not straightforward.
Yamane Intrascleral Haptic Fixation
After Shin Yamane, MD, presented his double-needle intrascleral haptic fixation (ISHF) technique in 2016, it was rapidly and widely adopted. The haptics of a three-piece IOL are externalized transconjunctivally through 27- or 30-gauge needles and heat-cauterized into flanges that lock themselves within oblique scleral tunnels. This technique requires no sutures, scleral flaps, or peritomy. In experienced hands, it is efficient and can be adapted easily to simultaneous vitreoretinal work.
Haptic material selection is critical. Polyvinylidene fluoride haptics, such as those of the CT Lucia (model 602, Carl Zeiss Meditec), are resilient during docking but have been associated with unexpected postoperative optic-haptic junction rotation that can produce clinically significant lens tilt, occasionally requiring endolaser refixation or an IOL exchange.4 PMMA haptics are more brittle but produce broader, more stable flanges. The most technically demanding moment is the haptic docking step; some surgeons prefer 30-gauge thin-walled needles for the smaller, more stable tunnels they create.
A fundamental constraint of the Yamane ISHF technique is that it requires a three-piece IOL. Any one-piece monoblock lens already in the eye must be explanted before ISHF can be performed.
Canabrava Double-Flanged Technique
Silas Canabrava, MD, extended the flanged sutureless principle to a polypropylene suture system that threads through IOL haptic eyelets and flanges after scleral externalization. The principal advantage of this approach over Yamane ISHF is broader compatibility: The Canabrava technique can fixate nonfoldable one-piece PMMA lenses; IOL–capsular bag complexes, including those with capsular tension rings; and even artificial irises.
In a prospective case series of 71 eyes, patients’ mean UCVA improved from 0.95 to 0.45 logMAR with more than 28 months’ follow-up.5 Flange-related complications occurred in approximately 13% of the 173 flanges, including sub-Tenon flange malposition in 7.5%, flange exposure in 2.89%, and late flange internalization in 2.2%; these accounted for most reoperations.5 Accurate flange burial is pivotal to a good result, and it demands care and patience that unexpected intraoperative scenarios do not always allow.
Glued IOL Technique
Pioneered by Amar Agarwal, MD, and practiced extensively across Asia and elsewhere, the glued IOL technique externalizes three-piece IOL haptics through opposing scleral flaps and seals them with fibrin glue, eliminating scleral sutures and maintaining the haptics’ anatomic position beneath protected tissue. The glued technique allows simultaneous access to the posterior segment. Mean IOL tilt has been reported at approximately 2.9° to 3.2° in published series.6
Practical constraints of this technique include fibrin glue availability, the time required to create and close scleral flaps, and the need for a usable conjunctival surface—criteria not always met by complex referral eyes.
A Purposefully Designed Option: The Carlevale IOL
My training allowed me to watch what happens when a fixation technique’s limitations are exposed by a complicated eye. In that situation, the Carlevale IOL (FIL SSF, Soleko) was often the preferred approach for secondary fixation thanks to its durability.
This one-piece foldable hydrophilic acrylic IOL has a 13.2-mm overall diameter and a 6.5-mm optic. T-shaped plugs project from the haptics and anchor the lens intrasclerally without sutures or glue; depending on the implantation technique, the plugs are seated beneath scleral flaps or within scleral pockets. The haptics carry a 5° anterior angulation to minimize iris contact and reduce the risk of pupillary block. The power range is -5.00 to +35.00 D, with a toric model that can address up to 10.00 D of corneal astigmatism simultaneously, a rare option among scleral-fixated lenses.7 The lens can be delivered through a 2.2-mm corneal incision via a dedicated Viscoject injector (Medicel), and the handshake technique allows self-centering without tactile optic manipulation.
Published series have consistently reported mean IOL tilt of approximately 2.1°, no endophthalmitis in several cohorts, and visual rehabilitation across diverse indications, including dislocated IOLs, PXF, trauma, and Marfan syndrome.7 A 2024 surgical modification eliminated scleral flaps by using the same vitrectomy sclerotomies for haptic delivery, which may reduce the total number of required scleral incisions and hypotony risk.8 Hypotony on postoperative day 1, frequent in early series, has generally been self-limited without meaningfully affecting final visual outcomes.
The implantation technique has a manageable learning curve and does not require sutures or glue. The lens is compatible with concurrent posterior segment surgery.
WHAT IS COMING NEXT
The Carlevale IOL demonstrates a principle that is driving the next generation of innovation: a fixation platform designed from the ground up can produce more predictable results than an IOL adapted to a purpose for which it was not engineered. Two emerging devices extend this concept in different directions.
The first is the prosthetic capsular bag (PCB; LensOne, Long Bridge Medical), for which a first-in-human multicenter trial was published online in April.9 The PCB is a ring delivered through a standard IOL injector, with or without a preloaded IOL, and anchored to the sclera through three fixation arms without sutures or scleral pockets. Conceptually, the device re-creates the anatomy of the capsular bag instead of bypassing it. In 15 patients lacking capsular or zonular support, there were no incidents of conjunctival erosion or IOL dislocation at 12 months, their UCVA improved by a mean of 12 lines, and their mean spherical equivalent was +0.12 D. This refractive precision is notable in eyes without a capsular reference. One patient with Marfan syndrome required secondary surgery for footplate reinternalization. The PCB’s three-arm fixation geometry is structurally distinct from existing two-haptic designs and could provide additional antitilt stability, but larger studies are needed to confirm this potential advantage.
The second device is the investigational Oseguera Ring (Eyedictive; Figures 1 and 2), which I developed to address a gap that neither the Carlevale IOL nor the PCB fills: a patient who already has a functionally adequate IOL that requires stabilization but not removal.10 Two concentric biocompatible polymer rings in the Oseguera Ring form an internal channel that capture the optic of an existing one- or three-piece posterior chamber IOL. The IOL’s haptics engage through a diagonal locking slot and an open slot with a single rotational maneuver. Two scleral haptics, offset approximately 2 mm from the device’s geometric centerline in opposite directions, are externalized through transscleral tunnels at the 3 and 9 clock positions without sutures. The design is intended to distribute fixation forces more evenly and reduce tilt, and ex vivo porcine testing has supported this concept. The Oseguera Ring can be compressed for delivery through a clear corneal incision smaller than 3.2 mm and is projected to cost less than US$15 per unit.
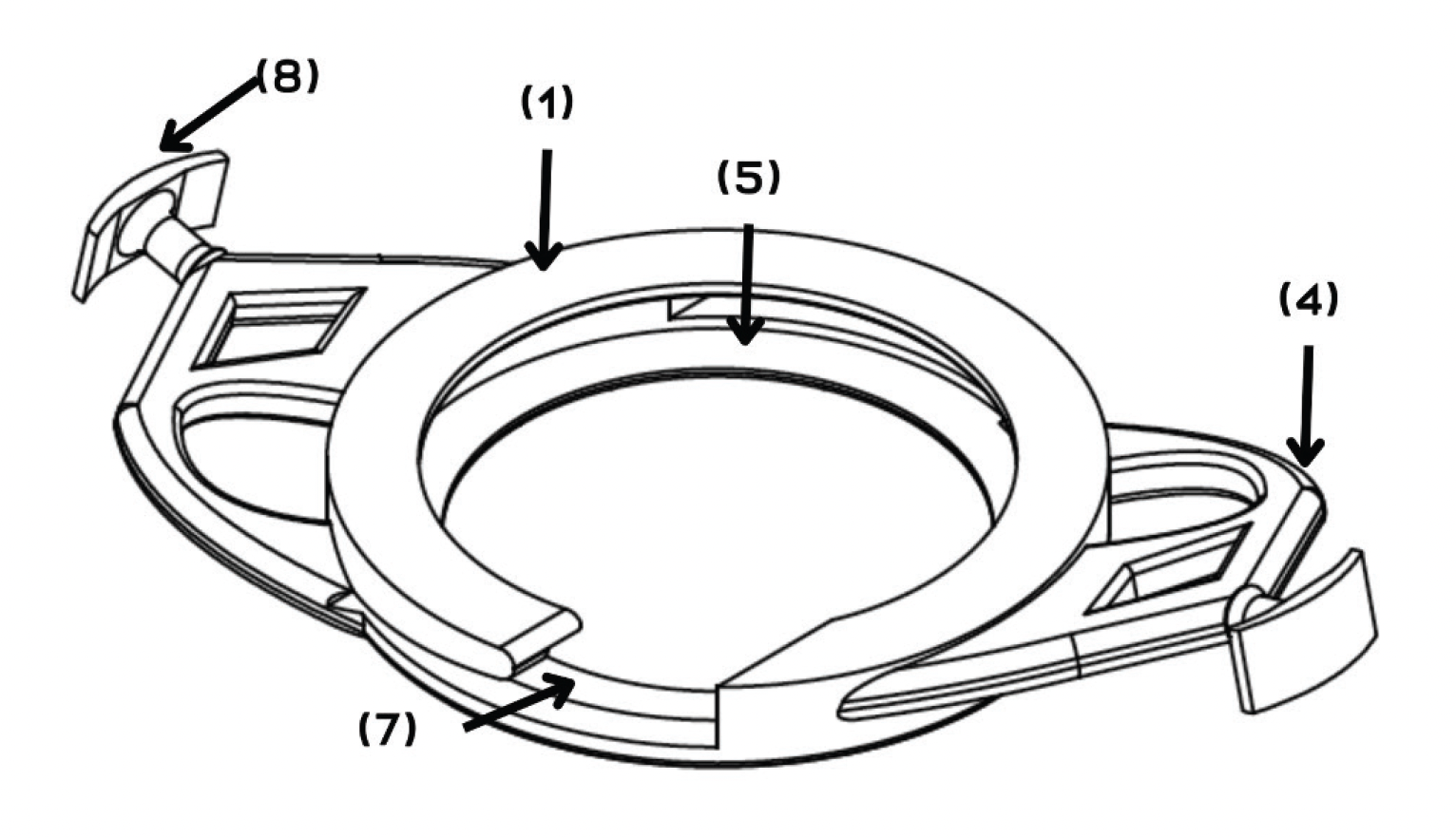
Figure 1. Isometric technical illustration of the Oseguera Ring. Superior ring (outer concentric ring; internal diameter, approximately 6.5 mm), which, together with the inferior ring, forms the IOL optic stabilization channel (1). Off-center scleral fixation haptic (right), offset approximately 2 mm from the device’s geometric centerline to create a biomechanical lever arm intended to counter tilt (4). Internal optic channel (interring groove; 0.8- to 1.5-mm spacing), designed to house the optic of a previously implanted posterior chamber IOL (5). Open slot (simplified nonrotational entry port for the second IOL haptic) (7). Scleral anchor (left haptic terminus; flexible plug designed for sutureless transscleral tunnel fixation at the 3 and 9 clock positions) (8). The anteriorly angulated haptic arms (10°–15°) are designed to minimize contact with the posterior iris and ciliary structures.
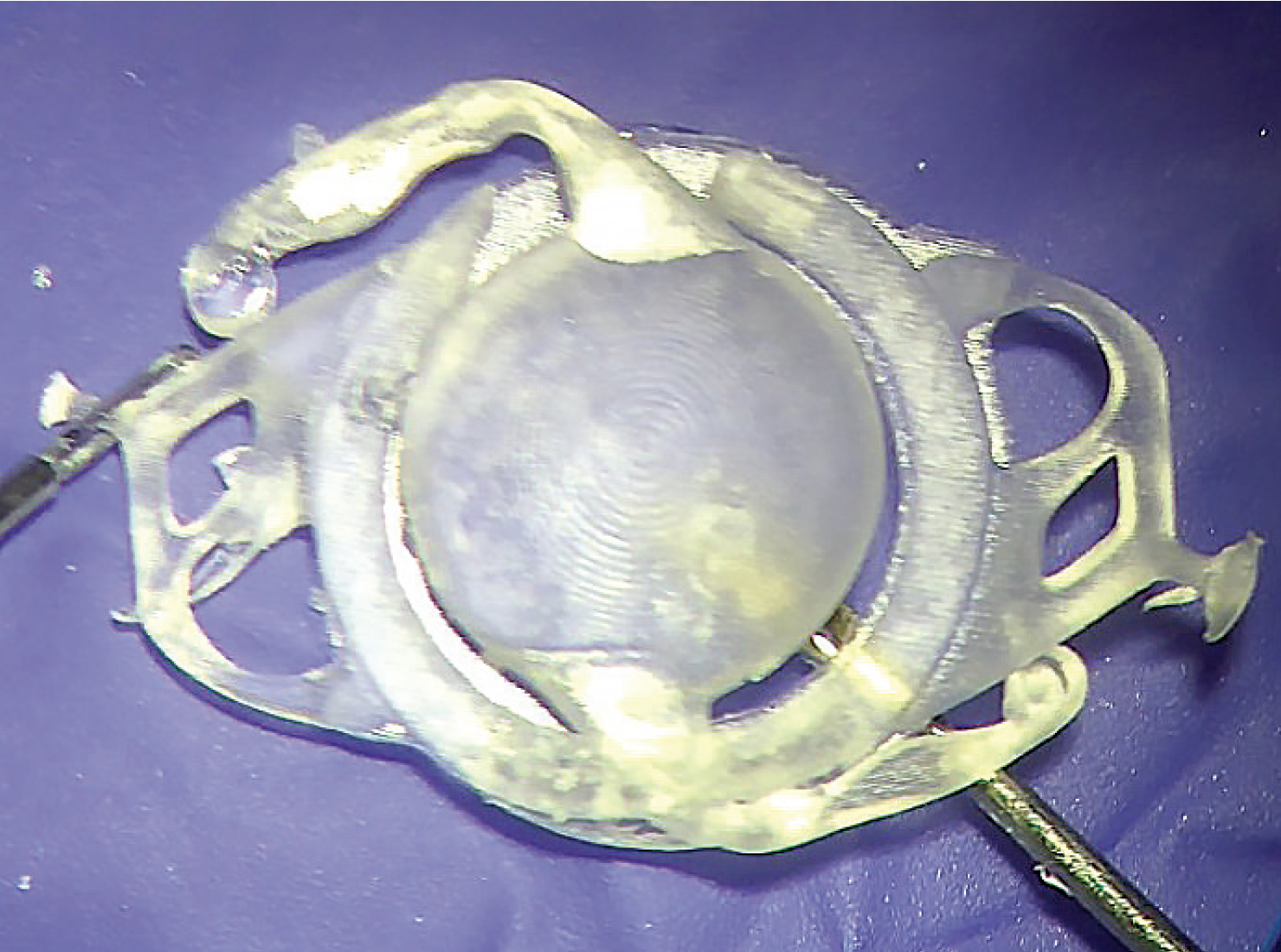
Figure 2. A 3D-printed prototype of the Oseguera Ring with a one-piece acrylic posterior chamber IOL docked within the interring optic channel. The IOL optic (center) is seated between the superior and inferior rings, and the concentric ring structure is visible surrounding the optic periphery. Two surgical instruments at left and right demonstrate the intended positioning of the scleral fixation haptics along the horizontal meridian, corresponding to transscleral externalization at the 3 and 9 clock positions. The diagonal locking slot in the upper-left quadrant and the open slot at the lower pole are visible at opposing poles. This bench model was used to evaluate one-step haptic engagement and optic centration before ex vivo porcine eye testing.
During cataract surgery, if the posterior capsule ruptures and a three-piece IOL is not available or if late subluxation of an optically adequate monoblock lens occurs, leaving the lens in a mechanically precarious position, currently, explantation of the lens is generally required. The Oseguera Ring may offer an alternative: stabilization of the existing lens. Clinical trials are planned as the device advances through industrial prototyping and regulatory evaluation.
The Table summarizes the practical characteristics of each approach described in this article.
CONCLUSION
Secondary IOL fixation has evolved from technically demanding sutured procedures to sutureless platforms delivered through wounds of less than 3 mm. The progression from polypropylene sutures prone to erosion to the Yamane technique for flanged ISHF, the Canabrava adaptation, and the self-centering T-haptic design of the Carlevale IOL has addressed the gaps in surgical options.
The goal is always to deliver the best possible visual outcome with the device already in the eye or the one to be implanted.
An AI language model (Claude Sonnet 4.6, Anthropic) was used to assist with language editing and manuscript structure. All content was reviewed, verified, and revised by the author, who assumes full responsibility for the accuracy and integrity of the manuscript. The AI tool was not used for data analysis, interpretation, or drawing scientific conclusions.
1. Tripathi M, Rao S, Sinha R. Scleral-fixated IOLs—a comprehensive review of current practices and emerging trends. Indian J Ophthalmol. 2025;73(7):933-945.
2. Shen JF, Deng S, Hammersmith KM, et al. Intraocular lens implantation in the absence of zonular support: an outcomes and safety update: a report by the American Academy of Ophthalmology. Ophthalmology. 2020;127(9):1234-1258.
3. Scleral fixated intraocular lens. EyeWiki. American Academy of Ophthalmology. Updated December 16, 2025. Accessed May 5, 2026. https://eyewiki.org/Scleral_Fixated_Intraocular_Lens
4. Safran JP, Safran SG. Intraocular lens tilt due to optic-haptic junction distortion following intrascleral haptic fixation with the Yamane technique. Am J Ophthalmol Case Rep. 2023;30:101845.
5. Canabrava S, Carvalho MS. Double-flanged polypropylene technique: 5-year results. J Cataract Refract Surg. 2023;49(6):565-570.
6. Kumar DA, Agarwal A, Agarwal A, Chandrasekar R, Priyanka V. Long-term assessment of tilt of glued intraocular lenses: an optical coherence tomography analysis 5 years after surgery. Ophthalmology. 2015;122(1):48-55.
7. Carlà MM, Boselli F, Giannuzzi F, et al. Sutureless scleral fixation Carlevale IOL: a review on the novel designed lens. Int Ophthalmol. 2023;43(6):2129-2138.
8. Danese C, Di Bin F, Lanzetta P. A mini-invasive surgical technique for Carlevale IOL implantation: case series study and description of concomitant surgery. Graefes Arch Clin Exp Ophthalmol. 2024;262(2):487-494.
9. Brodie FL, Naseri A, Ho IV, et al. Clinical outcomes of a prosthetic capsular bag for scleral fixation of an intraocular lens in eyes without capsular support. Ophthalmology. Published online April 24, 2026. doi:10.1016/j.ophtha.2026.04.021
10. López Oseguera G, inventor. Sutureless fixation device for stabilization of pre-implanted intraocular lenses (Oseguera Ring). PCT international patent application PCT/IB2025/055430. June 5, 2025.
